Alexia G Aguilar, Priscilla C Canals, Maria Tian, Kimberly A Miller, Brian J Piper
{"title":"Decreases and Pronounced Geographic Variability in Antibiotic Prescribing in Medicaid.","authors":"Alexia G Aguilar, Priscilla C Canals, Maria Tian, Kimberly A Miller, Brian J Piper","doi":"10.3390/pharmacy12020046","DOIUrl":null,"url":null,"abstract":"<p><p>Antibiotic resistance is a persistent and growing concern. Our objective was to analyze antibiotic prescribing in the United States (US) in the Medical Expenditure Panel System (MEPS) and to Medicaid patients. We obtained MEPS prescriptions for eight antibiotics from 2013 to 2020. We extracted prescribing rates per 1000 Medicaid enrollees for two years, 2018 and 2019, for four broad-spectrum (azithromycin, ciprofloxacin, levofloxacin, and moxifloxacin) and four narrow-spectrum (amoxicillin, cephalexin, doxycycline, and trimethoprim-sulfamethoxazole) antibiotics. Antibiotic prescriptions in MEPS decreased from 2013 to 2020 by 38.7%, with a larger decline for the broad (-53.7%) than narrow (-23.5%) spectrum antibiotics. Antibiotic prescriptions in Medicaid decreased by 6.7%. Amoxicillin was the predominant antibiotic, followed by azithromycin, cephalexin, trimethoprim-sulfamethoxazole, doxycycline, ciprofloxacin, levofloxacin, and moxifloxacin. Substantial geographic variation in prescribing existed, with a 2.8-fold difference between the highest (Kentucky = 855/1000) and lowest (Oregon = 299) states. The South prescribed 52.2% more antibiotics (580/1000) than the West (381/1000). There were significant correlations across states (r = 0.81 for azithromycin and amoxicillin). This study identified sizable disparities by geography in the prescribing rates of eight antibiotics with over three-fold state-level differences. Areas with high prescribing rates, particularly for outpatients, may benefit from stewardship programs to reduce potentially unnecessary prescribing.</p>","PeriodicalId":30544,"journal":{"name":"Pharmacy","volume":"12 2","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10961814/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pharmacy12020046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
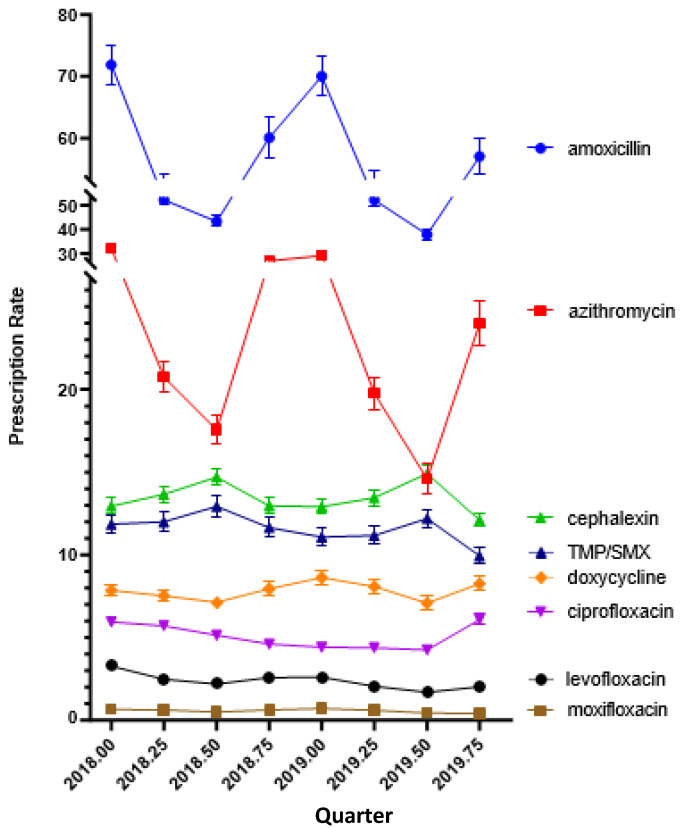
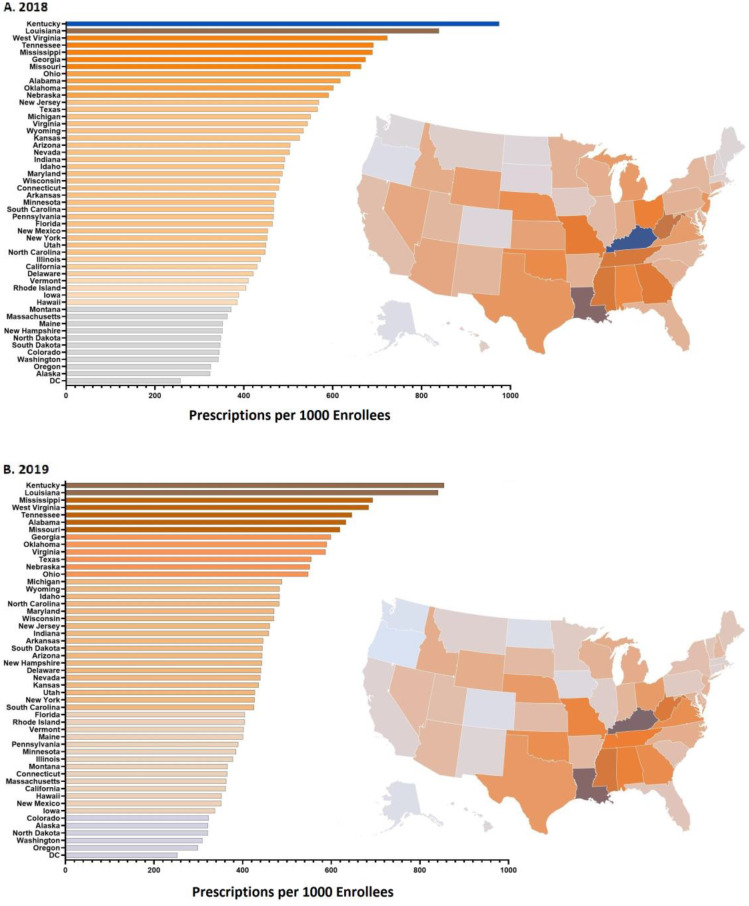
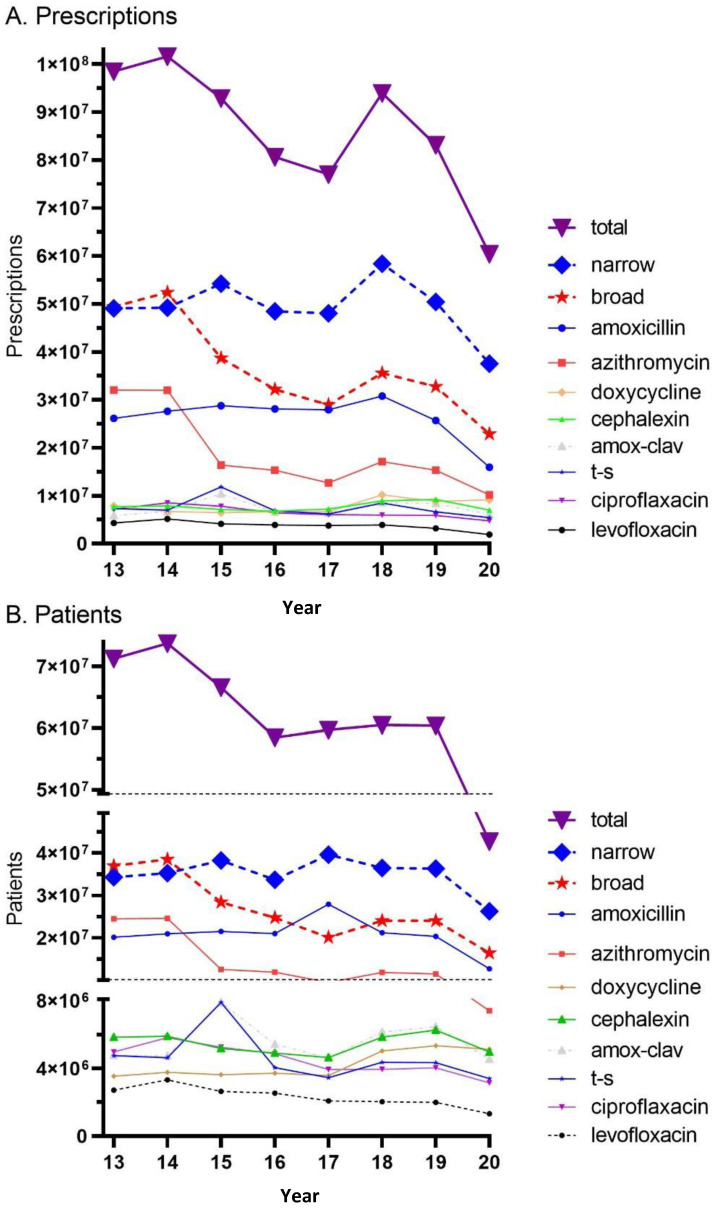
Antibiotic resistance is a persistent and growing concern. Our objective was to analyze antibiotic prescribing in the United States (US) in the Medical Expenditure Panel System (MEPS) and to Medicaid patients. We obtained MEPS prescriptions for eight antibiotics from 2013 to 2020. We extracted prescribing rates per 1000 Medicaid enrollees for two years, 2018 and 2019, for four broad-spectrum (azithromycin, ciprofloxacin, levofloxacin, and moxifloxacin) and four narrow-spectrum (amoxicillin, cephalexin, doxycycline, and trimethoprim-sulfamethoxazole) antibiotics. Antibiotic prescriptions in MEPS decreased from 2013 to 2020 by 38.7%, with a larger decline for the broad (-53.7%) than narrow (-23.5%) spectrum antibiotics. Antibiotic prescriptions in Medicaid decreased by 6.7%. Amoxicillin was the predominant antibiotic, followed by azithromycin, cephalexin, trimethoprim-sulfamethoxazole, doxycycline, ciprofloxacin, levofloxacin, and moxifloxacin. Substantial geographic variation in prescribing existed, with a 2.8-fold difference between the highest (Kentucky = 855/1000) and lowest (Oregon = 299) states. The South prescribed 52.2% more antibiotics (580/1000) than the West (381/1000). There were significant correlations across states (r = 0.81 for azithromycin and amoxicillin). This study identified sizable disparities by geography in the prescribing rates of eight antibiotics with over three-fold state-level differences. Areas with high prescribing rates, particularly for outpatients, may benefit from stewardship programs to reduce potentially unnecessary prescribing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


