Trent Edward Rayment, Sophie Williams, Alison Claire Jones
{"title":"A new height contouring method for severity prediction in cam-type hip joints: 20 subject-specific cases","authors":"Trent Edward Rayment, Sophie Williams, Alison Claire Jones","doi":"10.1016/j.bea.2024.100119","DOIUrl":null,"url":null,"abstract":"<div><p>Cam-type femoroacetabular impingement syndrome (FAIS) is characterised by a non-spherical continuation of the femoral head into the femoral head-neck junction and is associated with damage to the acetabular cartilage. Diagnostic methods based on cam shape are progressing from 2D radiographic measurements to 3D CT measures, providing greater insight. There is currently no consensus on how to describe the 3D cam lesion shape and subject-specific impingement mechanisms are difficult to determine.</p><p>A novel 3D ‘contour’ method was used to describe the proximal femur of 20 cam-type hips. Five contours, analogous to height contours on a terrain map, were used to describe the femoral head-neck junction, capturing the progressive height of the cam lesion. From that description, the <em>cam apex</em> (a subject's largest alpha angle), <em>cam extent</em> (spread around the femoral head), <em>cam location</em> (position around the femoral head) and <em>average acetabular coverage</em>, were recorded. A previously developed hip impingement model was used to apply 126 activity-based motions to each subject-specific hip shape and predict impingement occurrence and depth of incursion past the acetabular rim. Correlations between shape measures and impingement occurrence were investigated.</p><p>The two contours representing the lowest heights (close to the head best fit sphere and 1 mm greater than that) generated cam alpha angle and cam extent measurements which contained the typical clinical measures (Alpha: close to best fit 47°-98°, at 1 mm 45°–77°; Extent: close to best fit 0°–129°, at 1 mm 0°–100°). The remaining contours described the progressive height of the cam lesion up to 4 mm greater than the head radius. Impingement was predicted predominantly from the first 1 mm height of the cam, with only two subjects impinging at a cam height greater than 2 mm. Therefore, it is possible that adequate resection of the first 1 mm of cam height is the most critical in reducing a subject's impingement severity.</p><p>Impingement occurrence was positively correlated with the cam apex (ρ = 0.84 close to best fit, ρ = 0.70 at 1 mm height), the cam extent (ρ = 0.68 close to best fit, ρ = 0.80 at 1 mm height) and the acetabular coverage (ρ = 0.50, at 1 mm height). However, in line with other work on cam impingement, correlations between any single shape measure and the risk of impingement were not strong enough to be used with confidence as predictive tools. This supports the further development of modelling tools which sufficiently capture the complex shape and can generate an impingement risk metric which accounts for joint motion.</p></div>","PeriodicalId":72384,"journal":{"name":"Biomedical engineering advances","volume":"7 ","pages":"Article 100119"},"PeriodicalIF":0.0000,"publicationDate":"2024-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2667099224000082/pdfft?md5=18172cefad7057360bce393040d2aaff&pid=1-s2.0-S2667099224000082-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedical engineering advances","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667099224000082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Cam-type femoroacetabular impingement syndrome (FAIS) is characterised by a non-spherical continuation of the femoral head into the femoral head-neck junction and is associated with damage to the acetabular cartilage. Diagnostic methods based on cam shape are progressing from 2D radiographic measurements to 3D CT measures, providing greater insight. There is currently no consensus on how to describe the 3D cam lesion shape and subject-specific impingement mechanisms are difficult to determine.
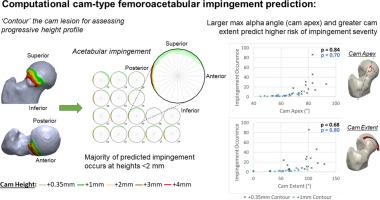
A novel 3D ‘contour’ method was used to describe the proximal femur of 20 cam-type hips. Five contours, analogous to height contours on a terrain map, were used to describe the femoral head-neck junction, capturing the progressive height of the cam lesion. From that description, the cam apex (a subject's largest alpha angle), cam extent (spread around the femoral head), cam location (position around the femoral head) and average acetabular coverage, were recorded. A previously developed hip impingement model was used to apply 126 activity-based motions to each subject-specific hip shape and predict impingement occurrence and depth of incursion past the acetabular rim. Correlations between shape measures and impingement occurrence were investigated.
The two contours representing the lowest heights (close to the head best fit sphere and 1 mm greater than that) generated cam alpha angle and cam extent measurements which contained the typical clinical measures (Alpha: close to best fit 47°-98°, at 1 mm 45°–77°; Extent: close to best fit 0°–129°, at 1 mm 0°–100°). The remaining contours described the progressive height of the cam lesion up to 4 mm greater than the head radius. Impingement was predicted predominantly from the first 1 mm height of the cam, with only two subjects impinging at a cam height greater than 2 mm. Therefore, it is possible that adequate resection of the first 1 mm of cam height is the most critical in reducing a subject's impingement severity.
Impingement occurrence was positively correlated with the cam apex (ρ = 0.84 close to best fit, ρ = 0.70 at 1 mm height), the cam extent (ρ = 0.68 close to best fit, ρ = 0.80 at 1 mm height) and the acetabular coverage (ρ = 0.50, at 1 mm height). However, in line with other work on cam impingement, correlations between any single shape measure and the risk of impingement were not strong enough to be used with confidence as predictive tools. This supports the further development of modelling tools which sufficiently capture the complex shape and can generate an impingement risk metric which accounts for joint motion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


