Lotte Bruyninckx, Serge Jennes, Jean-Paul Pirnay, Jean-Charles de Schoutheete
{"title":"Burn or trauma scoring: experience of the burn unit of the Queen Astrid Military Hospital during the terror attacks on 22 March 2016.","authors":"Lotte Bruyninckx, Serge Jennes, Jean-Paul Pirnay, Jean-Charles de Schoutheete","doi":"10.1007/s00068-024-02486-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>On 22 March 2016, the burn unit (BU) of Queen Astrid Military Hospital assessed a surge in severely injured victims from terror attacks at the national airport and Maalbeek subway station according to the damage control resuscitation (DCR) and damage control surgery (DCS) principles. This study delves into its approach to identify a suitable triage scoring system and to determine if a BU can serve as buffer capacity for mass casualty incidents (MCIs).</p><p><strong>Methods: </strong>The study reviewed retrospectively the origin of explosion, demographic data, sustained injuries, performed surgery, and length of stay of all admitted patients. Trauma scores (Injury Severity Score (ISS) and New Injury Severity Score (NISS)) and triage scores (Revised Trauma Score (RTS), New Trauma Score (NTS), and Trauma Score Injury Severity Score (TRISS)), were compared to burn mortality scores (Osler updated Baux Score and Tobiasen's Abbreviated Burn Severity Index (ABSI)).</p><p><strong>Results: </strong>Of the 23 casualties admitted to the BU, the scores calculated on average 3.5 indications for a level 1 trauma center (ISS 4, NISS 6, RTS 0, T-NTS 4). Nevertheless, no deaths occurred during admission or the 1-year follow-up.</p><p><strong>Conclusion: </strong>MCIs create chaos and a high demand for care. Avoiding bottlenecks and adhering to the DCR/DCS principles are necessary to deliver the best care to the largest number of people. This study indicates that a BU can serve as buffer capacity for MCIs. Nevertheless, its integration into the medical resilience plan depends on accurate scoring, comprehensive care availability, and understanding of the DCR/DCS concept. NTS for triage seems the best fit for scoring polytrauma referrals to a BU during MCIs.</p>","PeriodicalId":12064,"journal":{"name":"European Journal of Trauma and Emergency Surgery","volume":" ","pages":"1611-1619"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Trauma and Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00068-024-02486-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: On 22 March 2016, the burn unit (BU) of Queen Astrid Military Hospital assessed a surge in severely injured victims from terror attacks at the national airport and Maalbeek subway station according to the damage control resuscitation (DCR) and damage control surgery (DCS) principles. This study delves into its approach to identify a suitable triage scoring system and to determine if a BU can serve as buffer capacity for mass casualty incidents (MCIs).
Methods: The study reviewed retrospectively the origin of explosion, demographic data, sustained injuries, performed surgery, and length of stay of all admitted patients. Trauma scores (Injury Severity Score (ISS) and New Injury Severity Score (NISS)) and triage scores (Revised Trauma Score (RTS), New Trauma Score (NTS), and Trauma Score Injury Severity Score (TRISS)), were compared to burn mortality scores (Osler updated Baux Score and Tobiasen's Abbreviated Burn Severity Index (ABSI)).
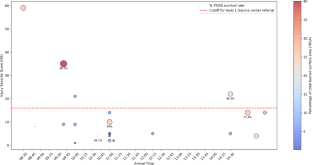
Results: Of the 23 casualties admitted to the BU, the scores calculated on average 3.5 indications for a level 1 trauma center (ISS 4, NISS 6, RTS 0, T-NTS 4). Nevertheless, no deaths occurred during admission or the 1-year follow-up.
Conclusion: MCIs create chaos and a high demand for care. Avoiding bottlenecks and adhering to the DCR/DCS principles are necessary to deliver the best care to the largest number of people. This study indicates that a BU can serve as buffer capacity for MCIs. Nevertheless, its integration into the medical resilience plan depends on accurate scoring, comprehensive care availability, and understanding of the DCR/DCS concept. NTS for triage seems the best fit for scoring polytrauma referrals to a BU during MCIs.
期刊介绍:
The European Journal of Trauma and Emergency Surgery aims to open an interdisciplinary forum that allows for the scientific exchange between basic and clinical science related to pathophysiology, diagnostics and treatment of traumatized patients. The journal covers all aspects of clinical management, operative treatment and related research of traumatic injuries.
Clinical and experimental papers on issues relevant for the improvement of trauma care are published. Reviews, original articles, short communications and letters allow the appropriate presentation of major and minor topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


