Current clinical evidence is insufficient to support HMME–PDT as the first choice of treatment for young children with port wine birthmarks
Abstract
Background
Port wine birthmark (PWB) is a congenital vascular malformation of the skin. Pulsed dye laser (PDL) is the “gold standard” for the treatment of PWB globally. Hematoporphyrin monomethyl ether (HMME or hemoporfin)-mediated photodynamic therapy (HMME–PDT) has emerged as the first choice for PWB treatment, particularly for young children, in many major hospitals in China during the past several decades.
Aim
To evaluate whether HMME–PDT is superior to PDL by comparing the clinical efficacies of both modalities.
Method
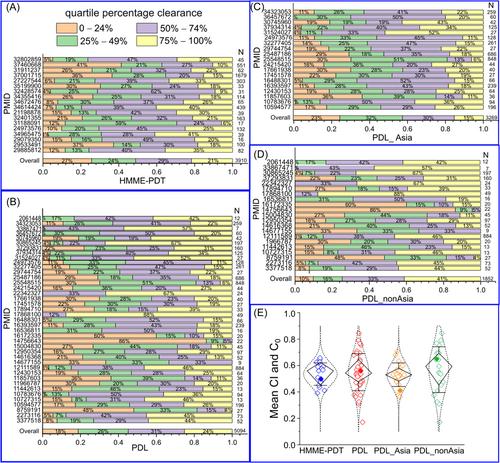
PubMed records were searched for all relevant studies of PWB treatment using PDL (1988−2023) or HMME–PDT (2007−2023). Patient characteristics and clinical efficacies were extracted. Studies with a quartile percentage clearance or similar scale were included. A mean color clearance index (CI) per study was calculated and compared among groups. An overall CI (C0), with data weighted by cohort size, was used to evaluate the final efficacy for each modality.
Result
A total of 18 HMME–PDT studies with 3910 patients in China were eligible for inclusion in this analysis. Similarly, 40 PDL studies with 5094 patients from nine different countries were eligible for inclusion in this analysis. Over 58% of patients in the HMME-PDT studies were minors (<18 years old). A significant portion (21.3%) were young children (<3 years old). Similarly, 33.2% of patients in the PDL studies were minors. A small proportion (9.3%) was young children. The overall clearance rates for PDL were slightly, but not significantly, higher than those for HMME–PDT in cohorts with patients of all ages (C0, 0.54 vs. 0.48, p = 0.733), subpopulations with only minors (C0, 0.54 vs. 0.46, p = 0.714), and young children (C0, 0.67 vs. 0.50, p = 0.081). Regrettably, there was a lack of long-term data on follow-up evaluations for efficacy and impact of HMME-PDT on young children in general, and central nervous system development in particular, because their blood-brain barriers have a greater permeability as compared to adults.
Conclusion
PDL shows overall albeit insignificantly higher clearance rates than HMME-PDT in patients of all ages; particularly statistical significance is nearly achieved in young children. Collectively, current evidence is insufficient to support HMME–PDT as the first choice of treatment of PWBs in young children given: (1) overall inferior efficacy as compared to PDL; (2) risk of off-target exposure to meningeal vasculature during the procedure; (3) administration of steriods for mitigation of side effects; -and (4) lack of long-term data on the potential impact of HMME on central nervous system development in young children.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


