Tal Perluk, Eiman Abu Bandora, Ophir Freund, Tommy Jacob, Inbal Friedman Regev, Eyal Kleinhendler, Michal Shteinberg, Amir Bar-Shai, Yael Oestriecher-Kedem
{"title":"Asymptomatic Dysphagia and Aspiration in Patients with Idiopathic Bronchiectasis.","authors":"Tal Perluk, Eiman Abu Bandora, Ophir Freund, Tommy Jacob, Inbal Friedman Regev, Eyal Kleinhendler, Michal Shteinberg, Amir Bar-Shai, Yael Oestriecher-Kedem","doi":"10.1007/s00408-024-00683-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Although considered contributors to idiopathic bronchiectasis (IB), neither dysphagia nor silent aspiration have been systematically evaluated in IB patients. We aimed to explore the prevalence of asymptomatic dysphagia and silent aspiration in IB patients and to identify parameters predictive of their presence.</p><p><strong>Methods: </strong>This prospective cohort study included IB patients from our Pulmonary Institute without prior history of dysphagia and without prior dysphagia workup. Swallowing function was assessed by the Eating Assessment Tool (EAT-10) questionnaire and by the Fiberoptic Endoscopic Evaluation of Swallowing (FEES) test.</p><p><strong>Results: </strong>Forty-seven patients (31 females, mean age 67 ± 16 years) were recruited. An EAT-10 score ≥ 3 (risk for swallowing problems) was present in 21 patients (44.6%). Forty-two patients (89.3%) had at least one abnormal swallowing parameter in the FEES test. Six patients (12.7%) had a penetration aspiration score (PAS) in the FEES of at least 6, indicating aspiration. An EAT-10 score of 3 was found to be the ideal cutoff to predict aspiration in the FEES, with a good level of accuracy (area under the curve = 0.78, 95% CI 0.629-0.932, p = 0.03) and sensitivity of 83%. This cutoff also showed a trend towards a more severe disease using the FACED (forced expiratory volume, age, colonization with pseudomonas, extension of lung involvement, dyspnea) score (p = 0.05).</p><p><strong>Conclusion: </strong>Dysphagia is prevalent in IB and may be undiagnosed if not specifically sought. We recommend screening all patients with IB for dysphagia by the EAT-10 questionnaire and referring all those with a score of ≥ 3 to formal swallowing assessment.</p>","PeriodicalId":18163,"journal":{"name":"Lung","volume":" ","pages":"189-195"},"PeriodicalIF":4.6000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11009759/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lung","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00408-024-00683-5","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/18 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Although considered contributors to idiopathic bronchiectasis (IB), neither dysphagia nor silent aspiration have been systematically evaluated in IB patients. We aimed to explore the prevalence of asymptomatic dysphagia and silent aspiration in IB patients and to identify parameters predictive of their presence.
Methods: This prospective cohort study included IB patients from our Pulmonary Institute without prior history of dysphagia and without prior dysphagia workup. Swallowing function was assessed by the Eating Assessment Tool (EAT-10) questionnaire and by the Fiberoptic Endoscopic Evaluation of Swallowing (FEES) test.
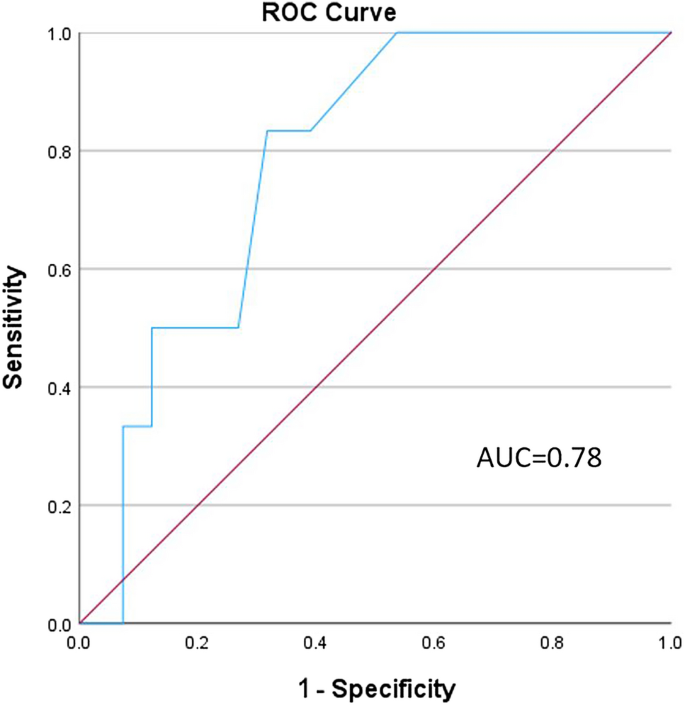
Results: Forty-seven patients (31 females, mean age 67 ± 16 years) were recruited. An EAT-10 score ≥ 3 (risk for swallowing problems) was present in 21 patients (44.6%). Forty-two patients (89.3%) had at least one abnormal swallowing parameter in the FEES test. Six patients (12.7%) had a penetration aspiration score (PAS) in the FEES of at least 6, indicating aspiration. An EAT-10 score of 3 was found to be the ideal cutoff to predict aspiration in the FEES, with a good level of accuracy (area under the curve = 0.78, 95% CI 0.629-0.932, p = 0.03) and sensitivity of 83%. This cutoff also showed a trend towards a more severe disease using the FACED (forced expiratory volume, age, colonization with pseudomonas, extension of lung involvement, dyspnea) score (p = 0.05).
Conclusion: Dysphagia is prevalent in IB and may be undiagnosed if not specifically sought. We recommend screening all patients with IB for dysphagia by the EAT-10 questionnaire and referring all those with a score of ≥ 3 to formal swallowing assessment.
期刊介绍:
Lung publishes original articles, reviews and editorials on all aspects of the healthy and diseased lungs, of the airways, and of breathing. Epidemiological, clinical, pathophysiological, biochemical, and pharmacological studies fall within the scope of the journal. Case reports, short communications and technical notes can be accepted if they are of particular interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


