Thomas Heisser, Carlo Senore, Michael Hoffmeister, Lina Jansen, Hermann Brenner
{"title":"Disclosing the true impact of screening endoscopy in colorectal cancer prevention","authors":"Thomas Heisser, Carlo Senore, Michael Hoffmeister, Lina Jansen, Hermann Brenner","doi":"10.1002/cac2.12531","DOIUrl":null,"url":null,"abstract":"<p>Preprint: https://doi.org/10.1101/2022.11.22.22282622</p><p>Randomized trials, cohort and modeling studies have consistently demonstrated a major impact of screening endoscopies on reducing colorectal cancer (CRC) incidence and mortality [<span>1</span>]. Over time, CRC mortality starts to be lower in those who underwent screening compared to those who did not due to earlier detection of prevalent, preclinical (asymptomatic) cases and lowering incidence through removing precancerous lesions. By contrast, measured incidence shows an initial apparent increase in the screening group due to the detection of preclinical (i.e., already prevalent) cancer. Only after around 4-6 years of follow-up, the measured cumulative incidence also starts to be lower in the screening group due to later manifestation of the initially preclinical cases in the control group and removal of precancerous lesions in the screening group [<span>2-6</span>].</p><p>However, measured incidence rates do not reflect true incidence rates as they are a mix of truly incident cases and cases that are already prevalent in the preclinical stage at baseline. As screening endoscopies cannot prevent prevalent CRC cases (but only remove precursor lesions at risk of developing into CRC), the commonly measured and reported effects on CRC incidence do not quantify the true endoscopy impact on CRC incidence, i.e., the impact on preventing newly developing CRC cases. In the present study, we sought to quantify the true impact of screening endoscopy on CRC incidence.</p><p>First, by re-calibrating the Colorectal Cancer Multistate Simulation Model (COSIMO), a thoroughly validated modeling approach, we replicated the Screening for COlon REctum trial (SCORE), a large, randomized trial (<i>n</i> = 34,292) examining the effect of a single flexible sigmoidoscopy in reducing CRC incidence and mortality by matching the numbers of simulated subjects and allocation per group with reported baseline numbers by sex and age, also taking into account colonoscopy referral and background endoscopy use [<span>5</span>]. Further details are provided in the Supplementary Material and Methods. The primary validation objective was the agreement between modeled and in SCORE reported incidence rate ratios (in the following: incidence rate ratio [unadjusted], IRR<sub>Unadjusted</sub>). The results were considered consistent if modeled estimates were within the 95% confidence intervals of the corresponding outcomes reported for SCORE.</p><p>Then, to determine the impact of prevalent preclinical CRCs on IRR<sub>Unadjusted</sub>, we calculated the adjusted IRR (incidence rate ratio (adjusted), IRR<sub>Adjusted</sub>, excluding prevalent CRCs at baseline) for the screening versus control groups by omitting the sex- and age-specific number of cases arising from prevalent preclinical CRC from the model calculation of IRRs for each year of follow-up.</p><p>Incidence rates and IRR<sub>Unadjusted</sub> predicted by COSIMO followed analogous patterns as those reported for SCORE (Figure 1A), i.e., in the first six years after randomization, the cumulative incidence in the screening group was higher than in the control group. All primary validation targets were reached (Supplementary Figure S1).</p><p>Excluding prevalent preclinical CRC at baseline markedly changed the numbers of detected CRC cases and incidence rates. The relative share of prevalent screen-detected cases among all detected cases was higher in the screening group than in the control group but exceeded 50% in the initial five years of follow-up in both groups (Figure 1B). The share of prevalent cases from all cumulatively reported cases diminished with increasing length of follow-up, but even after 15 years of follow-up, it was still as high as 22.5% and 17.5% in the screening and control groups, respectively.</p><p>In the intention-to-screen analysis, unadjusted/adjusted risk reductions after 8, 11 and 15 years of follow-up were 16%/31%, 20%/28%, and 21%/25%, respectively (Supplementary Table S1, Figure 1C). In per-protocol analyses, respective unadjusted/adjusted risk reductions were 28%/54%, 34%/49%, and 35%/44% (Figure 1D). Even though both IRR<sub>Unadjusted</sub> and IRR<sub>Adjusted</sub> were lower than 1, indicating a protective effect of screening, after 5 or more years of follow-up, and the difference between IRR<sub>Unadjusted</sub> and IRR<sub>Adjusted</sub> diminished over time, adjusted incidence reduction was still underestimated by 16% and 20% in intention-to-screen and per-protocol analyses, respectively, even after 15 years of follow-up.</p><p>The effectiveness of screening sigmoidoscopy to reduce CRC risks has been studied in four randomized controlled trials (RCTs), with reported cumulative incidence reductions after median 14-17 years of follow-up ranging from 18% to 26% in the intention-to-screen analysis and from 33% to 35% in the per-protocol analysis [<span>2-5</span>]. All RCTs have in common that the preventive effect of screening sigmoidoscopy (by removal of precancerous lesions following their endoscopic detection) mostly manifested after 4-6 years. Although the reason for this behavior (i.e., the dominance of screen-detected prevalent cancers, which could not any longer be prevented in the first years of follow-up) has been previously noted [<span>7, 8</span>], to our knowledge, no attempt has been made to quantify the impact of these prevalent cancers, and their relative contribution to the overall reported incidence reduction remained unclear.</p><p>This modeling study adds such quantification of the true impact of endoscopy on CRC incidence reduction to the literature. The findings indicate that the preventive potential of screening endoscopy is likely much larger than previously reported, most notably within the first 10 years after screening and still not fully discernable even after 15 years of follow-up. Excluding prevalent cancers had several implications. First, there was no characteristic crossing of incidence curves after 4-6 years [<span>2-5</span>], and the screening group was strongly favored from the beginning. Second, while the IRR<sub>Unadjusted</sub> tended to improve in favor of screening with increasing duration of follow-up, IRR<sub>Adjusted</sub> suggested the strongest difference between screening versus control early after screening. Still, strong differences were seen with increasing follow-up duration. Third, while IRR<sub>Adjusteds</sub> were consistently more favorable towards screening than IRR<sub>Unadjusted</sub>, the magnitude of the underestimation strongly depended on the time of follow-up (e.g., in intention-to-screen analyses, the “adjusted” incidence reduction by screening was 29 per cent points higher after 5 years, but only 4 per cent points higher after 15 years (Supplementary Table S1), illustrating the diminishing impact of prevalent preclinical cases with increasing follow-up durations.</p><p>Long-term outcomes from several RCTs on the effects of screening colonoscopy are still pending. Initial results from the Nordic-European Initiative on Colorectal Cancer trial (NordICC) were recently published [<span>6</span>]. However, given that follow-up so far was limited to 10 years, results are preliminary [<span>9</span>]. Our results suggest that the underestimation of true incidence reduction by the inclusion of a high proportion of prevalent cases may be substantial. The combined body of evidence from case-control, cohort and simulation studies suggests that the preventive potential of colonoscopy may even be larger than for sigmoidoscopy [<span>10</span>].</p><p>In summary, in randomized trials, the true impact of screening endoscopy on reducing CRC incidence is partly masked by the inclusion of preclinical (i.e., prevalent CRCs) at baseline. The relative share of such prevalent cases detected by screening from all detected cases strongly depends on the length of follow-up and diminishes over time. Excluding prevalent cancers at baseline in a replicated version of the randomized SCORE trial suggests that the “true” incidence reduction by screening sigmoidoscopy is strongly underestimated in the first 10 years of follow-up and still underestimated by 16%-20% even after 15 years compared to published estimates. Thus, the preventive effect of screening endoscopy is likely much stronger and manifests much earlier than previously reported. Published findings of randomized screening trials significantly underestimate the true preventive effects of screening endoscopy.</p><p>Hermann Brenner and Thomas Heisser designed the study and developed the methodology. Thomas Heisser conducted the statistical analyses and drafted the manuscript. All authors critically reviewed the manuscript, contributed to its revision, and approved the final version submitted. The researchers are independent from funders. All authors had full access to all of the data used for the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.</p><p>The authors declare no conflicts of interest.</p><p>Financial support for this study was provided in part by grants from the German Federal Ministry of Education and Research (grant numbers 01GL1712 and 01KD2104A) and the German Cancer Aid (grant number 70114735). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.</p><p>Not required.</p><p>Not required.</p><p>Not required.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 4","pages":"504-507"},"PeriodicalIF":20.1000,"publicationDate":"2024-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12531","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12531","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
Randomized trials, cohort and modeling studies have consistently demonstrated a major impact of screening endoscopies on reducing colorectal cancer (CRC) incidence and mortality [1]. Over time, CRC mortality starts to be lower in those who underwent screening compared to those who did not due to earlier detection of prevalent, preclinical (asymptomatic) cases and lowering incidence through removing precancerous lesions. By contrast, measured incidence shows an initial apparent increase in the screening group due to the detection of preclinical (i.e., already prevalent) cancer. Only after around 4-6 years of follow-up, the measured cumulative incidence also starts to be lower in the screening group due to later manifestation of the initially preclinical cases in the control group and removal of precancerous lesions in the screening group [2-6].
However, measured incidence rates do not reflect true incidence rates as they are a mix of truly incident cases and cases that are already prevalent in the preclinical stage at baseline. As screening endoscopies cannot prevent prevalent CRC cases (but only remove precursor lesions at risk of developing into CRC), the commonly measured and reported effects on CRC incidence do not quantify the true endoscopy impact on CRC incidence, i.e., the impact on preventing newly developing CRC cases. In the present study, we sought to quantify the true impact of screening endoscopy on CRC incidence.
First, by re-calibrating the Colorectal Cancer Multistate Simulation Model (COSIMO), a thoroughly validated modeling approach, we replicated the Screening for COlon REctum trial (SCORE), a large, randomized trial (n = 34,292) examining the effect of a single flexible sigmoidoscopy in reducing CRC incidence and mortality by matching the numbers of simulated subjects and allocation per group with reported baseline numbers by sex and age, also taking into account colonoscopy referral and background endoscopy use [5]. Further details are provided in the Supplementary Material and Methods. The primary validation objective was the agreement between modeled and in SCORE reported incidence rate ratios (in the following: incidence rate ratio [unadjusted], IRRUnadjusted). The results were considered consistent if modeled estimates were within the 95% confidence intervals of the corresponding outcomes reported for SCORE.
Then, to determine the impact of prevalent preclinical CRCs on IRRUnadjusted, we calculated the adjusted IRR (incidence rate ratio (adjusted), IRRAdjusted, excluding prevalent CRCs at baseline) for the screening versus control groups by omitting the sex- and age-specific number of cases arising from prevalent preclinical CRC from the model calculation of IRRs for each year of follow-up.
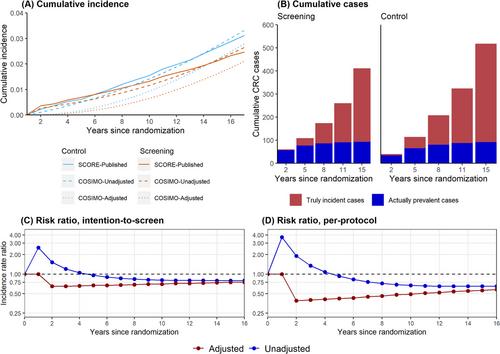
Incidence rates and IRRUnadjusted predicted by COSIMO followed analogous patterns as those reported for SCORE (Figure 1A), i.e., in the first six years after randomization, the cumulative incidence in the screening group was higher than in the control group. All primary validation targets were reached (Supplementary Figure S1).
Excluding prevalent preclinical CRC at baseline markedly changed the numbers of detected CRC cases and incidence rates. The relative share of prevalent screen-detected cases among all detected cases was higher in the screening group than in the control group but exceeded 50% in the initial five years of follow-up in both groups (Figure 1B). The share of prevalent cases from all cumulatively reported cases diminished with increasing length of follow-up, but even after 15 years of follow-up, it was still as high as 22.5% and 17.5% in the screening and control groups, respectively.
In the intention-to-screen analysis, unadjusted/adjusted risk reductions after 8, 11 and 15 years of follow-up were 16%/31%, 20%/28%, and 21%/25%, respectively (Supplementary Table S1, Figure 1C). In per-protocol analyses, respective unadjusted/adjusted risk reductions were 28%/54%, 34%/49%, and 35%/44% (Figure 1D). Even though both IRRUnadjusted and IRRAdjusted were lower than 1, indicating a protective effect of screening, after 5 or more years of follow-up, and the difference between IRRUnadjusted and IRRAdjusted diminished over time, adjusted incidence reduction was still underestimated by 16% and 20% in intention-to-screen and per-protocol analyses, respectively, even after 15 years of follow-up.
The effectiveness of screening sigmoidoscopy to reduce CRC risks has been studied in four randomized controlled trials (RCTs), with reported cumulative incidence reductions after median 14-17 years of follow-up ranging from 18% to 26% in the intention-to-screen analysis and from 33% to 35% in the per-protocol analysis [2-5]. All RCTs have in common that the preventive effect of screening sigmoidoscopy (by removal of precancerous lesions following their endoscopic detection) mostly manifested after 4-6 years. Although the reason for this behavior (i.e., the dominance of screen-detected prevalent cancers, which could not any longer be prevented in the first years of follow-up) has been previously noted [7, 8], to our knowledge, no attempt has been made to quantify the impact of these prevalent cancers, and their relative contribution to the overall reported incidence reduction remained unclear.
This modeling study adds such quantification of the true impact of endoscopy on CRC incidence reduction to the literature. The findings indicate that the preventive potential of screening endoscopy is likely much larger than previously reported, most notably within the first 10 years after screening and still not fully discernable even after 15 years of follow-up. Excluding prevalent cancers had several implications. First, there was no characteristic crossing of incidence curves after 4-6 years [2-5], and the screening group was strongly favored from the beginning. Second, while the IRRUnadjusted tended to improve in favor of screening with increasing duration of follow-up, IRRAdjusted suggested the strongest difference between screening versus control early after screening. Still, strong differences were seen with increasing follow-up duration. Third, while IRRAdjusteds were consistently more favorable towards screening than IRRUnadjusted, the magnitude of the underestimation strongly depended on the time of follow-up (e.g., in intention-to-screen analyses, the “adjusted” incidence reduction by screening was 29 per cent points higher after 5 years, but only 4 per cent points higher after 15 years (Supplementary Table S1), illustrating the diminishing impact of prevalent preclinical cases with increasing follow-up durations.
Long-term outcomes from several RCTs on the effects of screening colonoscopy are still pending. Initial results from the Nordic-European Initiative on Colorectal Cancer trial (NordICC) were recently published [6]. However, given that follow-up so far was limited to 10 years, results are preliminary [9]. Our results suggest that the underestimation of true incidence reduction by the inclusion of a high proportion of prevalent cases may be substantial. The combined body of evidence from case-control, cohort and simulation studies suggests that the preventive potential of colonoscopy may even be larger than for sigmoidoscopy [10].
In summary, in randomized trials, the true impact of screening endoscopy on reducing CRC incidence is partly masked by the inclusion of preclinical (i.e., prevalent CRCs) at baseline. The relative share of such prevalent cases detected by screening from all detected cases strongly depends on the length of follow-up and diminishes over time. Excluding prevalent cancers at baseline in a replicated version of the randomized SCORE trial suggests that the “true” incidence reduction by screening sigmoidoscopy is strongly underestimated in the first 10 years of follow-up and still underestimated by 16%-20% even after 15 years compared to published estimates. Thus, the preventive effect of screening endoscopy is likely much stronger and manifests much earlier than previously reported. Published findings of randomized screening trials significantly underestimate the true preventive effects of screening endoscopy.
Hermann Brenner and Thomas Heisser designed the study and developed the methodology. Thomas Heisser conducted the statistical analyses and drafted the manuscript. All authors critically reviewed the manuscript, contributed to its revision, and approved the final version submitted. The researchers are independent from funders. All authors had full access to all of the data used for the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
The authors declare no conflicts of interest.
Financial support for this study was provided in part by grants from the German Federal Ministry of Education and Research (grant numbers 01GL1712 and 01KD2104A) and the German Cancer Aid (grant number 70114735). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


