Azin Alizadehasl, Mina Mohseni, Kamran Roudini, Parisa Firoozbakhsh
{"title":"Trastuzumab in patients with breast cancer and pre-existing left ventricular systolic dysfunction.","authors":"Azin Alizadehasl, Mina Mohseni, Kamran Roudini, Parisa Firoozbakhsh","doi":"10.1186/s40959-024-00220-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Trastuzumab is one of the most effective treatments in HER-2 positive breast cancer patients. However, it is associated with development of cardiomyopathy/heart failure (HF) which is often a limiting side effect and associated with overall adverse outcomes. As a result, patients with pre-existing LV systolic dysfunction (LVSD) are often excluded from receiving anti-HER-2 therapy, which may lead to less effective cancer treatment and worse prognosis.</p><p><strong>Objectives: </strong>The current study aims to evaluate the safety of trastuzumab in patients with HER-2 positive breast cancer and pre-existing LVSD.</p><p><strong>Methods: </strong>In this retrospective cohort study, 36 consecutive patients at a single center in Iran with HER-2 positive breast cancer with asymptomatic mild LVSD with LVEF 40-53% without heart failure symptoms and those who were closely followed in the Cardio-Oncology clinic before initiating the treatment and then every two cycles of trastuzumab were included. As per the program standard protocol they received a beta-blocker (carvedilol) and ACE-I (Lisinopril), up to the maximum tolerated dose, if there were no contraindications. Patients underwent routine echocardiography with global longitudinal strain (GLS) assessment every 3 months per guideline recommendations and were followed up 6 months after the end of treatment. Primary composite outcomes included myocardial infarction (MI), cardiac arrhythmia, heart failure(HF) symptoms and cardiovascular death. Secondary outcome was ≥ 10% reduction in LVEF or ≥ 15% reduction in GLS compared to baseline. If the LVEF decreased below 40%, the treatment was temporarily interrupted for one or two cycles, and spironolactone was added to the patient's treatment. If the LVEF improved ≥ 40%, trastuzumab was rechallenged. Data analysis was performed using IBM SPSS Statistics 24.0. Software. Patients' characteristics were reported using descriptive statistics, and its association with drop in LVEF or GLS was assessed using Pearson chi-square or Mann-Whitney U test. A p-value of less than 0.05 was considered significant.</p><p><strong>Results: </strong>Thirty-six patients were included in the study. Primary composite outcome was noted in 1(2.8%) patient. LVEF reduction of ≥ 10% occurred in 6(16.7%) of the patients, and a GLS reduction of more than 15% was detected in 4 (11.1%) of the patients. There was a significant association between a ≥ 10% reduction in LVEF and baseline systolic blood pressure (P-value: 0.04). LVEF reduction below 40% was observed in 3 (8.3%) patients, where trastuzumab was interrupted. All of these three patients had obesity (Median BMI 34.11, IQR 9.12) and uncontrolled HTN, and one of them had symptoms of heart failure (NYHA class II), for whom the trastuzumab treatment was discontinued. Among two patients, after the temporary interruption of trastuzumab, and addition of spironolactone, LVEF improved to above 40%, and the treatment was restarted with close cardiac monitoring; therefore, they could complete the entire one-year treatment period.</p><p><strong>Conclusions: </strong>Treatment with trastuzumab seems to be safe in patients with pre-existing LVSD (LVEF = 40-53%). Such high-risk patients should be strictly monitored and cardiovascular risk factors, such as HTN should be regulated.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"10 1","pages":"16"},"PeriodicalIF":3.2000,"publicationDate":"2024-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10941531/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-024-00220-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Trastuzumab is one of the most effective treatments in HER-2 positive breast cancer patients. However, it is associated with development of cardiomyopathy/heart failure (HF) which is often a limiting side effect and associated with overall adverse outcomes. As a result, patients with pre-existing LV systolic dysfunction (LVSD) are often excluded from receiving anti-HER-2 therapy, which may lead to less effective cancer treatment and worse prognosis.
Objectives: The current study aims to evaluate the safety of trastuzumab in patients with HER-2 positive breast cancer and pre-existing LVSD.
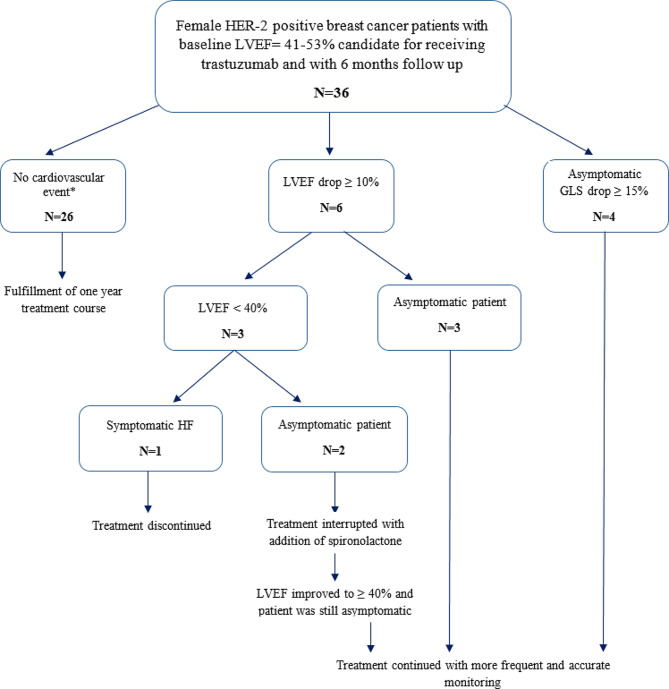
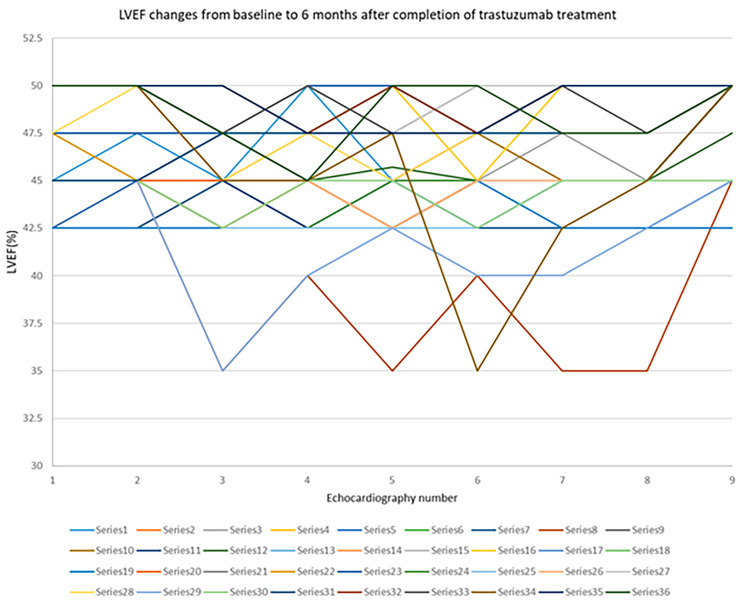
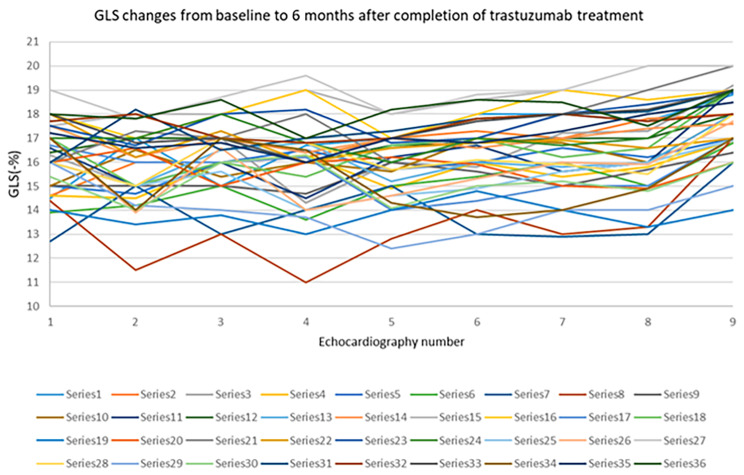
Methods: In this retrospective cohort study, 36 consecutive patients at a single center in Iran with HER-2 positive breast cancer with asymptomatic mild LVSD with LVEF 40-53% without heart failure symptoms and those who were closely followed in the Cardio-Oncology clinic before initiating the treatment and then every two cycles of trastuzumab were included. As per the program standard protocol they received a beta-blocker (carvedilol) and ACE-I (Lisinopril), up to the maximum tolerated dose, if there were no contraindications. Patients underwent routine echocardiography with global longitudinal strain (GLS) assessment every 3 months per guideline recommendations and were followed up 6 months after the end of treatment. Primary composite outcomes included myocardial infarction (MI), cardiac arrhythmia, heart failure(HF) symptoms and cardiovascular death. Secondary outcome was ≥ 10% reduction in LVEF or ≥ 15% reduction in GLS compared to baseline. If the LVEF decreased below 40%, the treatment was temporarily interrupted for one or two cycles, and spironolactone was added to the patient's treatment. If the LVEF improved ≥ 40%, trastuzumab was rechallenged. Data analysis was performed using IBM SPSS Statistics 24.0. Software. Patients' characteristics were reported using descriptive statistics, and its association with drop in LVEF or GLS was assessed using Pearson chi-square or Mann-Whitney U test. A p-value of less than 0.05 was considered significant.
Results: Thirty-six patients were included in the study. Primary composite outcome was noted in 1(2.8%) patient. LVEF reduction of ≥ 10% occurred in 6(16.7%) of the patients, and a GLS reduction of more than 15% was detected in 4 (11.1%) of the patients. There was a significant association between a ≥ 10% reduction in LVEF and baseline systolic blood pressure (P-value: 0.04). LVEF reduction below 40% was observed in 3 (8.3%) patients, where trastuzumab was interrupted. All of these three patients had obesity (Median BMI 34.11, IQR 9.12) and uncontrolled HTN, and one of them had symptoms of heart failure (NYHA class II), for whom the trastuzumab treatment was discontinued. Among two patients, after the temporary interruption of trastuzumab, and addition of spironolactone, LVEF improved to above 40%, and the treatment was restarted with close cardiac monitoring; therefore, they could complete the entire one-year treatment period.
Conclusions: Treatment with trastuzumab seems to be safe in patients with pre-existing LVSD (LVEF = 40-53%). Such high-risk patients should be strictly monitored and cardiovascular risk factors, such as HTN should be regulated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


