{"title":"Adding MYC/BCL2 double expression to NCCN-IPI may not improve prognostic value to an acceptable level.","authors":"Naree Warnnissorn, Nonglak Kanitsap, Pimjai Niparuck, Paisarn Boonsakan, Prapasri Kulalert, Wasithep Limvorapitak, Lantarima Bhoopat, Supawee Saengboon, Chinnawut Suriyonplengsaeng, Pichika Chantrathammachart, Teeraya Puavilai, Suporn Chuncharunee","doi":"10.1007/s44313-024-00006-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>MYC/BCL2 double expression (DE) is associated with poor prognosis in patients with diffuse large B-cell lymphoma (DLBCL) receiving rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP). This study aimed to determine whether the addition of DE to the National Comprehensive Cancer Network Internal Prognostic Index (NCCN-IPI) could improve the prediction of disease progression in patients with DLBCL treated with R-CHOP.</p><p><strong>Methods: </strong>This confirmatory prognostic factor study retrospectively recruited patients with newly diagnosed DLBCL between January 1, 2014, and January 31, 2018, at Ramathibodi Hospital (RA) and Thammasat University Hospital (TU). The follow-up period ended on July 1, 2022. Tumors expressing MYC ≥ 40% and BCL2 ≥ 50% were classified as DE. We calculated the hazard ratios (HR) for progression-free survival (PFS) from the date of diagnosis to refractory disease, relapse, or death. Discrimination of the 5-year prediction was based on Cox models using Harrell's concordance index (c-index).</p><p><strong>Results: </strong>A total of 111 patients had DE (39%), NCCN-IPI (8%), and disease progression (46%). The NCCN-IPI adjusted HR of DE was 1.6 (95% confidence interval [CI]: 0.9-2.8; P = 0.117). The baseline NCCN-IPI c-index was 0.63. Adding DE to the NCCN-IPI slightly increased Harrell's concordance index (c-index) to 0.66 (P = 0.119).</p><p><strong>Conclusions: </strong>Adding DE to the NCCN-IPI may not improve the prognostic value to an acceptable level in resource-limited settings. Multiple independent confirmatory studies from a large cohort of lymphoma registries have provided additional evidence for the clinical utility of DE.</p>","PeriodicalId":46224,"journal":{"name":"Blood Research","volume":"59 1","pages":"2"},"PeriodicalIF":2.8000,"publicationDate":"2024-02-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10903517/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44313-024-00006-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: MYC/BCL2 double expression (DE) is associated with poor prognosis in patients with diffuse large B-cell lymphoma (DLBCL) receiving rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone (R-CHOP). This study aimed to determine whether the addition of DE to the National Comprehensive Cancer Network Internal Prognostic Index (NCCN-IPI) could improve the prediction of disease progression in patients with DLBCL treated with R-CHOP.
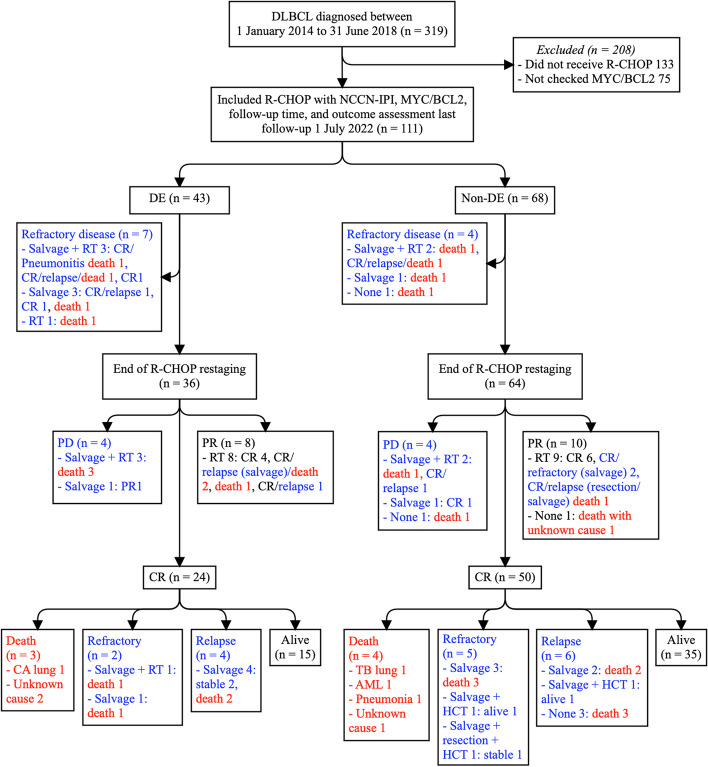
Methods: This confirmatory prognostic factor study retrospectively recruited patients with newly diagnosed DLBCL between January 1, 2014, and January 31, 2018, at Ramathibodi Hospital (RA) and Thammasat University Hospital (TU). The follow-up period ended on July 1, 2022. Tumors expressing MYC ≥ 40% and BCL2 ≥ 50% were classified as DE. We calculated the hazard ratios (HR) for progression-free survival (PFS) from the date of diagnosis to refractory disease, relapse, or death. Discrimination of the 5-year prediction was based on Cox models using Harrell's concordance index (c-index).
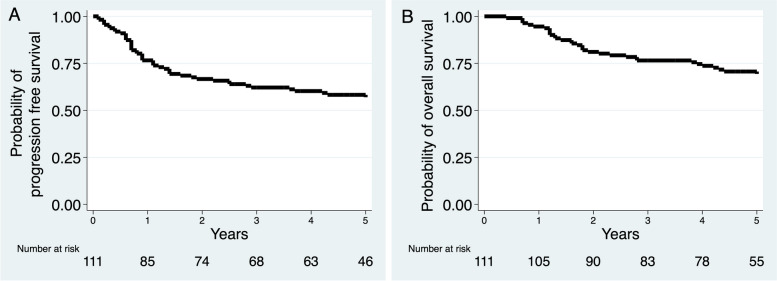
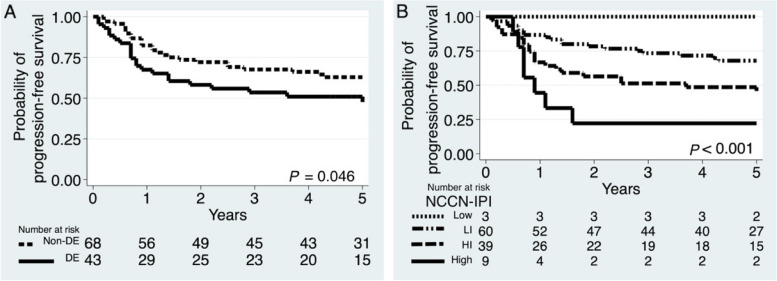
Results: A total of 111 patients had DE (39%), NCCN-IPI (8%), and disease progression (46%). The NCCN-IPI adjusted HR of DE was 1.6 (95% confidence interval [CI]: 0.9-2.8; P = 0.117). The baseline NCCN-IPI c-index was 0.63. Adding DE to the NCCN-IPI slightly increased Harrell's concordance index (c-index) to 0.66 (P = 0.119).
Conclusions: Adding DE to the NCCN-IPI may not improve the prognostic value to an acceptable level in resource-limited settings. Multiple independent confirmatory studies from a large cohort of lymphoma registries have provided additional evidence for the clinical utility of DE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


