{"title":"Role of source control in critically ill candidemic patients: a multicenter retrospective study.","authors":"Markos Marangos, Petros Ioannou, Laurence Senn, Anastasia Spiliopoulou, Sotiris Tzalis, Fevronia Kolonitsiou, Maria Valta, Sofia Kokkini, Jean-Luc Pagani, Dimitra Stafylaki, Fotini Paliogianni, Fotini Fligou, Diamantis P Kofteridis, Frédéric Lamoth, Matthaios Papadimitriou-Olivgeris","doi":"10.1007/s15010-024-02222-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Candidemia is associated with high mortality especially in critically ill patients. Our aim was to identify predictors of mortality among critically ill patients with candidemia with a focus on early interventions that can improve prognosis.</p><p><strong>Methods: </strong>Multicenter retrospective study.</p><p><strong>Setting: </strong>This retrospective study was conducted in Intensive Care Units from three European university hospitals from 2015 to 2021. Adult patients with at least one positive blood culture for Candida spp. were included. Patients who did not require source control were excluded. Primary outcome was 14-day mortality.</p><p><strong>Results: </strong>A total of 409 episodes of candidemia were included. Most candidemias were catheter related (173; 41%), followed by unknown origin (170; 40%). Septic shock developed in 43% episodes. Overall, 14-day mortality rate was 29%. In Cox proportional hazards regression model, septic shock (P 0.001; HR 2.20, CI 1.38-3.50), SOFA score ≥ 10 points (P 0.008; HR 1.83, CI 1.18-2.86), and prior SARS-CoV-2 infection (P 0.003; HR 1.87, CI 1.23-2.85) were associated with 14-day mortality, while combined early appropriate antifungal treatment and source control (P < 0.001; HR 0.15, CI 0.08-0.28), and early source control without appropriate antifungal treatment (P < 0.001; HR 0.23, CI 0.12-0.47) were associated with better survival compared to those without neither early appropriate antifungal treatment nor source control.</p><p><strong>Conclusion: </strong>Early source control was associated with better outcome among candidemic critically ill patients.</p>","PeriodicalId":13600,"journal":{"name":"Infection","volume":null,"pages":null},"PeriodicalIF":5.4000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11499412/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infection","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s15010-024-02222-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/12 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Candidemia is associated with high mortality especially in critically ill patients. Our aim was to identify predictors of mortality among critically ill patients with candidemia with a focus on early interventions that can improve prognosis.
Methods: Multicenter retrospective study.
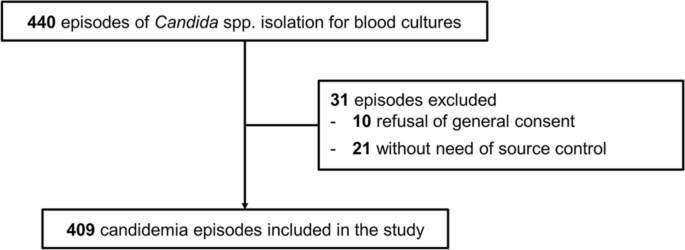
Setting: This retrospective study was conducted in Intensive Care Units from three European university hospitals from 2015 to 2021. Adult patients with at least one positive blood culture for Candida spp. were included. Patients who did not require source control were excluded. Primary outcome was 14-day mortality.
Results: A total of 409 episodes of candidemia were included. Most candidemias were catheter related (173; 41%), followed by unknown origin (170; 40%). Septic shock developed in 43% episodes. Overall, 14-day mortality rate was 29%. In Cox proportional hazards regression model, septic shock (P 0.001; HR 2.20, CI 1.38-3.50), SOFA score ≥ 10 points (P 0.008; HR 1.83, CI 1.18-2.86), and prior SARS-CoV-2 infection (P 0.003; HR 1.87, CI 1.23-2.85) were associated with 14-day mortality, while combined early appropriate antifungal treatment and source control (P < 0.001; HR 0.15, CI 0.08-0.28), and early source control without appropriate antifungal treatment (P < 0.001; HR 0.23, CI 0.12-0.47) were associated with better survival compared to those without neither early appropriate antifungal treatment nor source control.
Conclusion: Early source control was associated with better outcome among candidemic critically ill patients.
期刊介绍:
Infection is a journal dedicated to serving as a global forum for the presentation and discussion of clinically relevant information on infectious diseases. Its primary goal is to engage readers and contributors from various regions around the world in the exchange of knowledge about the etiology, pathogenesis, diagnosis, and treatment of infectious diseases, both in outpatient and inpatient settings.
The journal covers a wide range of topics, including:
Etiology: The study of the causes of infectious diseases.
Pathogenesis: The process by which an infectious agent causes disease.
Diagnosis: The methods and techniques used to identify infectious diseases.
Treatment: The medical interventions and strategies employed to treat infectious diseases.
Public Health: Issues of local, regional, or international significance related to infectious diseases, including prevention, control, and management strategies.
Hospital Epidemiology: The study of the spread of infectious diseases within healthcare settings and the measures to prevent nosocomial infections.
In addition to these, Infection also includes a specialized "Images" section, which focuses on high-quality visual content, such as images, photographs, and microscopic slides, accompanied by brief abstracts. This section is designed to highlight the clinical and diagnostic value of visual aids in the field of infectious diseases, as many conditions present with characteristic clinical signs that can be diagnosed through inspection, and imaging and microscopy are crucial for accurate diagnosis. The journal's comprehensive approach ensures that it remains a valuable resource for healthcare professionals and researchers in the field of infectious diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


