Fahimeh Talaei, Qi-Xuan Ang, Min-Choon Tan, Mustafa Hassan, Luis Scott, Yong-Mei Cha, Justin Z Lee, Kamala Tamirisa
{"title":"Impact of infective versus sterile transvenous lead removal on 30-day outcomes in cardiac implantable electronic devices.","authors":"Fahimeh Talaei, Qi-Xuan Ang, Min-Choon Tan, Mustafa Hassan, Luis Scott, Yong-Mei Cha, Justin Z Lee, Kamala Tamirisa","doi":"10.1007/s10840-024-01775-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transvenous lead removal (TLR) is associated with increased mortality and morbidity. This study sought to evaluate the impact of TLR on in-hospital mortality and outcomes in patients with and without CIED infection.</p><p><strong>Methods: </strong>From January 1, 2017, to December 31, 2020, we utilized the nationally representative, all-payer, Nationwide Readmissions Database to assess patients who underwent TLR. We categorized TLR as indicated for infection, if the patient had a diagnosis of bacteremia, sepsis, or endocarditis during the initial admission. Conversely, if none of these conditions were present, TLR was considered sterile. The impact of infective vs sterile indications of TLR on mortality and major adverse events was studied.</p><p><strong>Results: </strong>Out of the total 25,144 patients who underwent TLR, 14,030 (55.8%) received TLR based on sterile indications, while 11,114 (44.2%) received TLR due to device infection, with 40.5% having systemic infection and 59.5% having isolated pocket infection. TLR due to infective indications was associated with a significant in-hospital mortality (5.59% vs 1.13%; OR = 5.16; 95% CI 4.33-6.16; p < 0.001). Moreover, when compared with sterile indications, TLR performed due to device infection was associated with a considerable risk of thromboembolic events including pulmonary embolism and stroke (OR = 3.80; 95% CI 3.23-4.47, p < 0.001). However, there was no significant difference in the conversion to open heart surgery (1.72% vs. 1.47%, p < 0.111), and infection was not an independent predictor of cardiac (OR = 1.12; 95% CI 0.97-1.29) or vascular complications (OR = 1.12; 95% CI 0.73-1.72) between the two groups.</p><p><strong>Conclusion: </strong>Higher in-hospital mortality and rates of thromboembolic events associated with TLR resulting from infective indications may warrant further pursuing this diagnosis in patients.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"1517-1527"},"PeriodicalIF":2.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01775-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/9 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Transvenous lead removal (TLR) is associated with increased mortality and morbidity. This study sought to evaluate the impact of TLR on in-hospital mortality and outcomes in patients with and without CIED infection.
Methods: From January 1, 2017, to December 31, 2020, we utilized the nationally representative, all-payer, Nationwide Readmissions Database to assess patients who underwent TLR. We categorized TLR as indicated for infection, if the patient had a diagnosis of bacteremia, sepsis, or endocarditis during the initial admission. Conversely, if none of these conditions were present, TLR was considered sterile. The impact of infective vs sterile indications of TLR on mortality and major adverse events was studied.
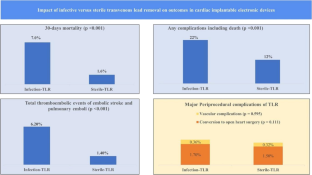
Results: Out of the total 25,144 patients who underwent TLR, 14,030 (55.8%) received TLR based on sterile indications, while 11,114 (44.2%) received TLR due to device infection, with 40.5% having systemic infection and 59.5% having isolated pocket infection. TLR due to infective indications was associated with a significant in-hospital mortality (5.59% vs 1.13%; OR = 5.16; 95% CI 4.33-6.16; p < 0.001). Moreover, when compared with sterile indications, TLR performed due to device infection was associated with a considerable risk of thromboembolic events including pulmonary embolism and stroke (OR = 3.80; 95% CI 3.23-4.47, p < 0.001). However, there was no significant difference in the conversion to open heart surgery (1.72% vs. 1.47%, p < 0.111), and infection was not an independent predictor of cardiac (OR = 1.12; 95% CI 0.97-1.29) or vascular complications (OR = 1.12; 95% CI 0.73-1.72) between the two groups.
Conclusion: Higher in-hospital mortality and rates of thromboembolic events associated with TLR resulting from infective indications may warrant further pursuing this diagnosis in patients.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


