{"title":"Advancing clinical practice and discovery research through revised taxonomy: Case in point bipolar disorder diagnosis","authors":"Anne Duffy, Paul Grof","doi":"10.1111/bdi.13415","DOIUrl":null,"url":null,"abstract":"<p>In the well-articulated paper by Malhi et al.<span><sup>1</sup></span> in this journal, several problems with diagnosing bipolar disorder in children are discussed and as rightly pointed out “impede our ability to conduct meaningful research and advance clinical practice”. In fact, one could argue that the diagnostic challenges outlined apply to the diagnoses of mood disorders more generally. That is, reliance on a diagnostic checklist that reflects largely non-specific symptoms that cross diagnostic boundaries and are open to interpretation yield a highly heterogeneous population of mood disordered patients that share the same diagnosis but little else—differing in clinical course, family history, prognosis, treatment response and genetic and neurobiological correlates.</p><p>Malhi et al. offer a novel solution to the current diagnostic dilemma. The authors express hope that revising the current taxonomy so as to focus on developmentally sensitive symptom clusters, reflecting the evolution of the disorder over development, will advance the field past the current stalemate and improve diagnostic accuracy. While we agree that a developmental lens provides an informative perspective through which to view psychopathology, there is no evidence that a sole focus on symptoms, no matter how well developmentally nuanced, will improve diagnostic classification. Rather, substantive evidence supports the need to identify more homogenous subtypes from within the current heterogeneous bipolar diagnostic construct to advance risk prediction, pharmacotherapy, and discovery research. Three bipolar subtypes based on distinct clinical profiles have been described based on research extending over six decades, each with preferential response to stabilizing treatment with lithium, antipsychotics and antiepileptics, respectively (Figure 1).<span><sup>2</sup></span> Therefore, an alternative evidence-based solution would be to include these bipolar subtypes in a revised taxonomy.</p><p>Specifically, substantive evidence supports that a long-term response to lithium identifies a more homogeneous subtype of bipolar disorder characterized by a recurrent episodic course, complete remission, a history of episodic mood disorders in family members, and distinctive genetic correlates.<span><sup>3</sup></span> This distinctive clinical profile, identified by multivariate analyses, was actually delineated by Kraepelin over a century ago. Further, prospective longitudinal studies of the offspring of lithium responsive (LiR) and lithium non-responsive (LiNR) bipolar parents have provided evidence that bipolar disorder debuts as a depressive episode in adolescence, years on average before emergence of the first manic episode.<span><sup>4</sup></span> The developmental history and clinical course differ between subgroups, with offspring of LiRs having normal or gifted development and offspring of LiNRs manifesting neurodevelopmental disorders (ADHD, learning difficulties). Childhood clinical antecedents predicting major mood disorders include anxiety and sleep disorders, which in the offspring of LiRs follow an episodic course, while in offspring of LiNRs are chronic or fluctuating with incomplete remission (Figure 2).<span><sup>4</sup></span> Further, the clinical course of mood disorders in offspring aligns with that of the parent; that is offspring of LiRs manifest episodic remitting mood disorders with stable functioning between episodes, while offspring of LiNRs manifest chronic or partial remitting mood disorders with lower global functioning over time.<span><sup>4</sup></span> Self-reported manic symptoms did not differentiate high-risk from control offspring (of well parents)—in fact, controls endorsed higher hypomanic symptom levels; however, hypomanic symptoms identified on clinical assessment did predict onset of mood disorders in high-risk offspring, while no clinically meaningful hypomania was identified in controls.<span><sup>5</sup></span></p><p>Taken together, longitudinal studies over decades of carefully prospectively studied adult bipolar patients and their relatives, including their children, have provided convergent evidence supporting bipolar subtypes that differ in characteristic developmental trajectories of emergent psychopathology, clinical course, prognosis, treatment response, and genetic and neurobiological correlates. This strongly suggests these clinical profiles index bipolar subtypes with shared genetic factors and pathophysiological mechanisms that differ meaningfully between subtypes. Therefore, we argue that a necessary revision to advance precision diagnosis that maps to preferential stabilizing treatment and reliably associated biomarkers rests on the incorporation of characteristic clinical profiles of bipolar subtypes into the diagnostic taxonomy. The clinical profiles, as illustrated briefly here, go beyond developmentally sensitive symptom clusters, which only have clinical meaning when considered in the context of a carefully detailed family history and clinical course.</p><p>Had the longitudinal evidence identifying characteristic clinical profiles of bipolar subtypes (including the developmental trajectories) been applied and incorporated in routine clinical practice, the entire debate about the validity of a pediatric (i.e. pre-pubertal mania) bipolar disorder equivalent might have been avoided or at least put to rest much earlier on. That said, lessons learned from the pediatric bipolar debate include that symptoms alone are insufficient evidence on which to rest a stable and accurate diagnosis, especially early in the emergent course. Further, as in other areas of medicine, the importance of a thorough clinical assessment that considers all predictive clinical information in the diagnostic formulation and includes collateral history and a carefully collected family history is paramount. While structured and semi-structured interviews and symptom checklists (developmentally sensitive or not) may be useful in large epidemiological studies, advances in psychiatry clinical practice and discovery research will require selective focus on carefully clinically characterized patients in order to identify those of the same bipolar subtype associated with a predictable course, preferential response to stabilizing treatment and shared pathogenesis.</p>","PeriodicalId":8959,"journal":{"name":"Bipolar Disorders","volume":"26 3","pages":"286-288"},"PeriodicalIF":5.0000,"publicationDate":"2024-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13415","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bipolar Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13415","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
In the well-articulated paper by Malhi et al.1 in this journal, several problems with diagnosing bipolar disorder in children are discussed and as rightly pointed out “impede our ability to conduct meaningful research and advance clinical practice”. In fact, one could argue that the diagnostic challenges outlined apply to the diagnoses of mood disorders more generally. That is, reliance on a diagnostic checklist that reflects largely non-specific symptoms that cross diagnostic boundaries and are open to interpretation yield a highly heterogeneous population of mood disordered patients that share the same diagnosis but little else—differing in clinical course, family history, prognosis, treatment response and genetic and neurobiological correlates.
Malhi et al. offer a novel solution to the current diagnostic dilemma. The authors express hope that revising the current taxonomy so as to focus on developmentally sensitive symptom clusters, reflecting the evolution of the disorder over development, will advance the field past the current stalemate and improve diagnostic accuracy. While we agree that a developmental lens provides an informative perspective through which to view psychopathology, there is no evidence that a sole focus on symptoms, no matter how well developmentally nuanced, will improve diagnostic classification. Rather, substantive evidence supports the need to identify more homogenous subtypes from within the current heterogeneous bipolar diagnostic construct to advance risk prediction, pharmacotherapy, and discovery research. Three bipolar subtypes based on distinct clinical profiles have been described based on research extending over six decades, each with preferential response to stabilizing treatment with lithium, antipsychotics and antiepileptics, respectively (Figure 1).2 Therefore, an alternative evidence-based solution would be to include these bipolar subtypes in a revised taxonomy.
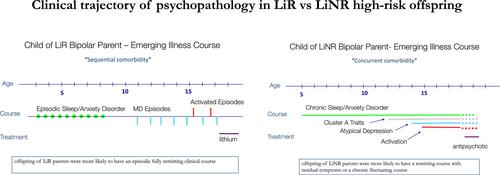
Specifically, substantive evidence supports that a long-term response to lithium identifies a more homogeneous subtype of bipolar disorder characterized by a recurrent episodic course, complete remission, a history of episodic mood disorders in family members, and distinctive genetic correlates.3 This distinctive clinical profile, identified by multivariate analyses, was actually delineated by Kraepelin over a century ago. Further, prospective longitudinal studies of the offspring of lithium responsive (LiR) and lithium non-responsive (LiNR) bipolar parents have provided evidence that bipolar disorder debuts as a depressive episode in adolescence, years on average before emergence of the first manic episode.4 The developmental history and clinical course differ between subgroups, with offspring of LiRs having normal or gifted development and offspring of LiNRs manifesting neurodevelopmental disorders (ADHD, learning difficulties). Childhood clinical antecedents predicting major mood disorders include anxiety and sleep disorders, which in the offspring of LiRs follow an episodic course, while in offspring of LiNRs are chronic or fluctuating with incomplete remission (Figure 2).4 Further, the clinical course of mood disorders in offspring aligns with that of the parent; that is offspring of LiRs manifest episodic remitting mood disorders with stable functioning between episodes, while offspring of LiNRs manifest chronic or partial remitting mood disorders with lower global functioning over time.4 Self-reported manic symptoms did not differentiate high-risk from control offspring (of well parents)—in fact, controls endorsed higher hypomanic symptom levels; however, hypomanic symptoms identified on clinical assessment did predict onset of mood disorders in high-risk offspring, while no clinically meaningful hypomania was identified in controls.5
Taken together, longitudinal studies over decades of carefully prospectively studied adult bipolar patients and their relatives, including their children, have provided convergent evidence supporting bipolar subtypes that differ in characteristic developmental trajectories of emergent psychopathology, clinical course, prognosis, treatment response, and genetic and neurobiological correlates. This strongly suggests these clinical profiles index bipolar subtypes with shared genetic factors and pathophysiological mechanisms that differ meaningfully between subtypes. Therefore, we argue that a necessary revision to advance precision diagnosis that maps to preferential stabilizing treatment and reliably associated biomarkers rests on the incorporation of characteristic clinical profiles of bipolar subtypes into the diagnostic taxonomy. The clinical profiles, as illustrated briefly here, go beyond developmentally sensitive symptom clusters, which only have clinical meaning when considered in the context of a carefully detailed family history and clinical course.
Had the longitudinal evidence identifying characteristic clinical profiles of bipolar subtypes (including the developmental trajectories) been applied and incorporated in routine clinical practice, the entire debate about the validity of a pediatric (i.e. pre-pubertal mania) bipolar disorder equivalent might have been avoided or at least put to rest much earlier on. That said, lessons learned from the pediatric bipolar debate include that symptoms alone are insufficient evidence on which to rest a stable and accurate diagnosis, especially early in the emergent course. Further, as in other areas of medicine, the importance of a thorough clinical assessment that considers all predictive clinical information in the diagnostic formulation and includes collateral history and a carefully collected family history is paramount. While structured and semi-structured interviews and symptom checklists (developmentally sensitive or not) may be useful in large epidemiological studies, advances in psychiatry clinical practice and discovery research will require selective focus on carefully clinically characterized patients in order to identify those of the same bipolar subtype associated with a predictable course, preferential response to stabilizing treatment and shared pathogenesis.
期刊介绍:
Bipolar Disorders is an international journal that publishes all research of relevance for the basic mechanisms, clinical aspects, or treatment of bipolar disorders and related illnesses. It intends to provide a single international outlet for new research in this area and covers research in the following areas:
biochemistry
physiology
neuropsychopharmacology
neuroanatomy
neuropathology
genetics
brain imaging
epidemiology
phenomenology
clinical aspects
and therapeutics of bipolar disorders
Bipolar Disorders also contains papers that form the development of new therapeutic strategies for these disorders as well as papers on the topics of schizoaffective disorders, and depressive disorders as these can be cyclic disorders with areas of overlap with bipolar disorders.
The journal will consider for publication submissions within the domain of: Perspectives, Research Articles, Correspondence, Clinical Corner, and Reflections. Within these there are a number of types of articles: invited editorials, debates, review articles, original articles, commentaries, letters to the editors, clinical conundrums, clinical curiosities, clinical care, and musings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


