Luciana Martel-Duguech, Jonathan Poirier, Isabelle Bourdeau, André Lacroix
{"title":"Diagnosis and management of secondary adrenal crisis.","authors":"Luciana Martel-Duguech, Jonathan Poirier, Isabelle Bourdeau, André Lacroix","doi":"10.1007/s11154-024-09877-x","DOIUrl":null,"url":null,"abstract":"<p><p>Adrenal crisis (AC) is a life threatening acute adrenal insufficiency (AI) episode which can occur in patients with primary AI but also secondary AI (SAI), tertiary AI (TAI) and iatrogenic AI (IAI). In SAI, TAI and IAI, AC may develop when the HPA axis is unable to mount an adequate glucocorticoid response to severe stress due to pituitary or hypothalamic disruption. It manifests as an acute deterioration in multi-organ homeostasis that, if untreated, leads to shock and death. Despite the availability of effective preventive strategies, its prevalence is increasing in patients with SAI, TAI and IAI due to more frequent exogenous steroid administration, pituitary immune-related effects of immune checkpoint inhibitors and opioid use in pain management. The delayed diagnosis of acute AI which remains infrequently suspected increases the risk of AC. Its main precipitating factors are infections, emotional distress, surgery, cessation or reduction in GC doses, pituitary infarction or surgical cure of endogenous Cushing's syndrome. In patients not known previously to have SAI/TAI/IAI, recognition of its symptoms, signs, and biochemical abnormalities can be challenging and cause delay in proper diagnosis and therapy. Effective therapy of AC is rapid intravenous administration of hydrocortisone (initial bolus of 100 mg followed by 200 mg/24 h as continuous infusion or bolus of 50 mg every 6 h) and 0.9% saline. In diagnosed patients, preventive education in sick-day rules adjustment of glucocorticoid replacement and hydrocortisone parenteral self-administration must be performed repeatedly by trained health care providers. Strategies to improve the adequate preventive education in patients at risk for secondary AI should be promoted in collaboration with various medical specialist societies and patients support associations.</p>","PeriodicalId":21106,"journal":{"name":"Reviews in Endocrine & Metabolic Disorders","volume":" ","pages":"619-637"},"PeriodicalIF":6.9000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reviews in Endocrine & Metabolic Disorders","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11154-024-09877-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
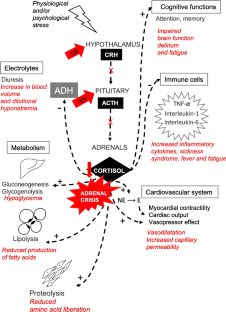
Adrenal crisis (AC) is a life threatening acute adrenal insufficiency (AI) episode which can occur in patients with primary AI but also secondary AI (SAI), tertiary AI (TAI) and iatrogenic AI (IAI). In SAI, TAI and IAI, AC may develop when the HPA axis is unable to mount an adequate glucocorticoid response to severe stress due to pituitary or hypothalamic disruption. It manifests as an acute deterioration in multi-organ homeostasis that, if untreated, leads to shock and death. Despite the availability of effective preventive strategies, its prevalence is increasing in patients with SAI, TAI and IAI due to more frequent exogenous steroid administration, pituitary immune-related effects of immune checkpoint inhibitors and opioid use in pain management. The delayed diagnosis of acute AI which remains infrequently suspected increases the risk of AC. Its main precipitating factors are infections, emotional distress, surgery, cessation or reduction in GC doses, pituitary infarction or surgical cure of endogenous Cushing's syndrome. In patients not known previously to have SAI/TAI/IAI, recognition of its symptoms, signs, and biochemical abnormalities can be challenging and cause delay in proper diagnosis and therapy. Effective therapy of AC is rapid intravenous administration of hydrocortisone (initial bolus of 100 mg followed by 200 mg/24 h as continuous infusion or bolus of 50 mg every 6 h) and 0.9% saline. In diagnosed patients, preventive education in sick-day rules adjustment of glucocorticoid replacement and hydrocortisone parenteral self-administration must be performed repeatedly by trained health care providers. Strategies to improve the adequate preventive education in patients at risk for secondary AI should be promoted in collaboration with various medical specialist societies and patients support associations.
期刊介绍:
Reviews in Endocrine and Metabolic Disorders is an international journal dedicated to the field of endocrinology and metabolism. It aims to provide the latest advancements in this rapidly advancing field to students, clinicians, and researchers. Unlike other journals, each quarterly issue of this review journal focuses on a specific topic and features ten to twelve articles written by world leaders in the field. These articles provide brief overviews of the latest developments, offering insights into both the basic aspects of the disease and its clinical implications. This format allows individuals in all areas of the field, including students, academic clinicians, and practicing clinicians, to understand the disease process and apply their knowledge to their specific areas of interest. The journal also includes selected readings and other essential references to encourage further in-depth exploration of specific topics.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


