{"title":"[Drug-resistant pulmonary tuberculosis at Maradi Regional Hospital Center, Niger (2014-2018)].","authors":"Mahaman Laouali Harouna Amadou, Ibrahim Maman Lawan, Ousmane Abdoulaye, Abdoul Kadir Ibrahim Mamadou, Oumarou Amadou, Hassane Boureima, Biraima Ahamadou, Nouhou Hama Aghali, Nana Hadiza Abdourahamane Maifada, Abdoulaziz Kabirou Amoussa, Chaibou Maidakouale","doi":"10.48327/mtsi.v3i4.2023.438","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim of study: </strong>To describe the clinical, therapeutic and evolutionary profile of patients followed for rifampicin-resistant pulmonary tuberculosis (RR-TB) at the Regional Hospital Centre (RHC) of Maradi (Niger) from 2014 to 2018.</p><p><strong>Methods: </strong>We conducted a retrospective and descriptive study based on the records of patients followed for Multidrug-resistant tuberculosis (MDR-TB) between January 1, 2014 and June 30, 2018 at the resistant tuberculosis management unit in Maradi (Niger). This unit is located within the RHC of Maradi and has a capacity of 20 beds in 4 wards. It receives patients with tuberculosis resistant to first-line anti-tuberculosis drugs. In this study, patients diagnosed with RR-TB by genotypic (GeneXpert MTB/RIF) or phenotypic (culture) testing were included. We excluded from this study: patients previously treated for more than 1 month with second-line anti-TB drugs; patients with resistance to second-line injectables (SLI) and/or fluoroquinolones (FQ); patients with an electrocardiogram QTc greater than 500 ms (the corrected QT (QTc) estimates the QT interval at a rate of 60 beats per second); cases of atypical mycobacteriosis detected by phenotypic testing.Patients were previously on 2RHZE/4RH prior to the discovery of resistance. The treatment protocol for resistant TB was as follows: 4KmMfxPtoCfzHZE/5MfxCfzZE (The second-line injectable was replaced by Lzd in case of initial or treatment-emergent deafness). HIV co-infected patients received, in addition to anti-tuberculosis drugs, antiretrovirals and cotrimoxazole in preventive doses.</p><p><strong>Results: </strong>A total of 80 patients were included in the present study (70 males and 10 females, mean age 34.4 years with extremes ranging from 18 to 71 years). Patients aged 18-35 years accounted for more than half. Patients with primary treatment failure were the most frequent type (36%) followed by patients with retreatment failure (24%) and patients with retreatment relapse (17%). It should be noted that 77 patients (96%) were previously treated for TB and only 3 patients (4%) were new cases. The majority of patients (70%) had a Body mass index of less than 18 kg/m<sup>2</sup>. 7.5% of patients were HIV positive, one was diabetic, 52% of the patients had grade 2 radiological lesions. Grade 1 deafness was noted at the beginning of treatment in 3%. A third of patients (36%) were primary treatment failures. The treatment protocol was as follows: 4KmMfxPtoCfzHZE/5MfxCfzZE. Only 1 patient had a positive culture at the end of the 4th month of treatment. Most of the patients had experienced adverse events, mainly digestive, with vomiting being the most common. The therapeutic success rate was 88%. We noted 10% of deaths, 1% of therapeutic failure and 1% of lost to follow-up.Six months after treatment, 48 patients (60%) were smear negative and 43 (54%) were culture negative. In 32 patients (40%), the smear was not performed and culture was not performed in 37.</p><p><strong>Conclusion: </strong>The short treatment regime gives satisfactory results in the absence of resistance to fluoroquinolones, with rare adverse effects. In Niger, further efforts should be made to minimize the delay in diagnosis which is responsible for most deaths during treatment. A centre could usefully be designated to organize \"TB consiliums\" allowing any practitioner to submit difficult cases of MDR-TB.</p>","PeriodicalId":101416,"journal":{"name":"Medecine tropicale et sante internationale","volume":"3 4","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-11-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10882245/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medecine tropicale et sante internationale","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.48327/mtsi.v3i4.2023.438","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/31 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aim of study: To describe the clinical, therapeutic and evolutionary profile of patients followed for rifampicin-resistant pulmonary tuberculosis (RR-TB) at the Regional Hospital Centre (RHC) of Maradi (Niger) from 2014 to 2018.
Methods: We conducted a retrospective and descriptive study based on the records of patients followed for Multidrug-resistant tuberculosis (MDR-TB) between January 1, 2014 and June 30, 2018 at the resistant tuberculosis management unit in Maradi (Niger). This unit is located within the RHC of Maradi and has a capacity of 20 beds in 4 wards. It receives patients with tuberculosis resistant to first-line anti-tuberculosis drugs. In this study, patients diagnosed with RR-TB by genotypic (GeneXpert MTB/RIF) or phenotypic (culture) testing were included. We excluded from this study: patients previously treated for more than 1 month with second-line anti-TB drugs; patients with resistance to second-line injectables (SLI) and/or fluoroquinolones (FQ); patients with an electrocardiogram QTc greater than 500 ms (the corrected QT (QTc) estimates the QT interval at a rate of 60 beats per second); cases of atypical mycobacteriosis detected by phenotypic testing.Patients were previously on 2RHZE/4RH prior to the discovery of resistance. The treatment protocol for resistant TB was as follows: 4KmMfxPtoCfzHZE/5MfxCfzZE (The second-line injectable was replaced by Lzd in case of initial or treatment-emergent deafness). HIV co-infected patients received, in addition to anti-tuberculosis drugs, antiretrovirals and cotrimoxazole in preventive doses.
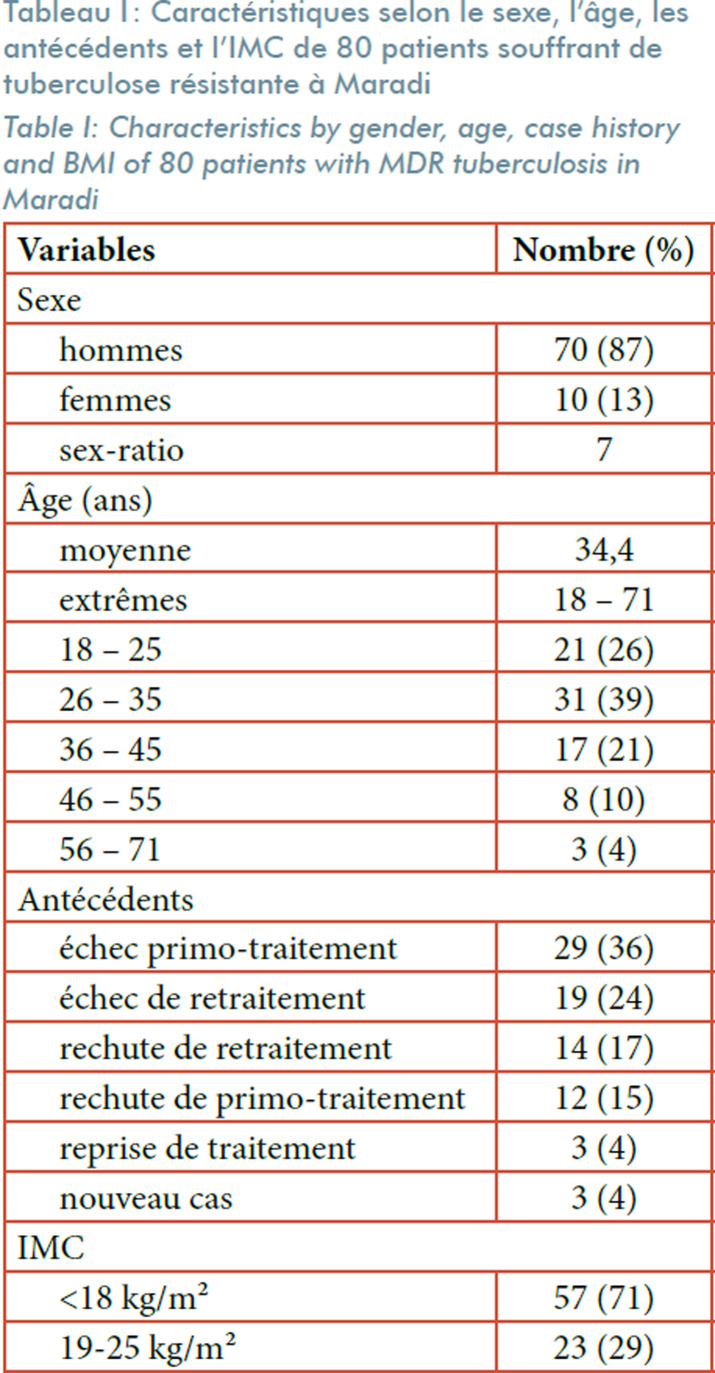
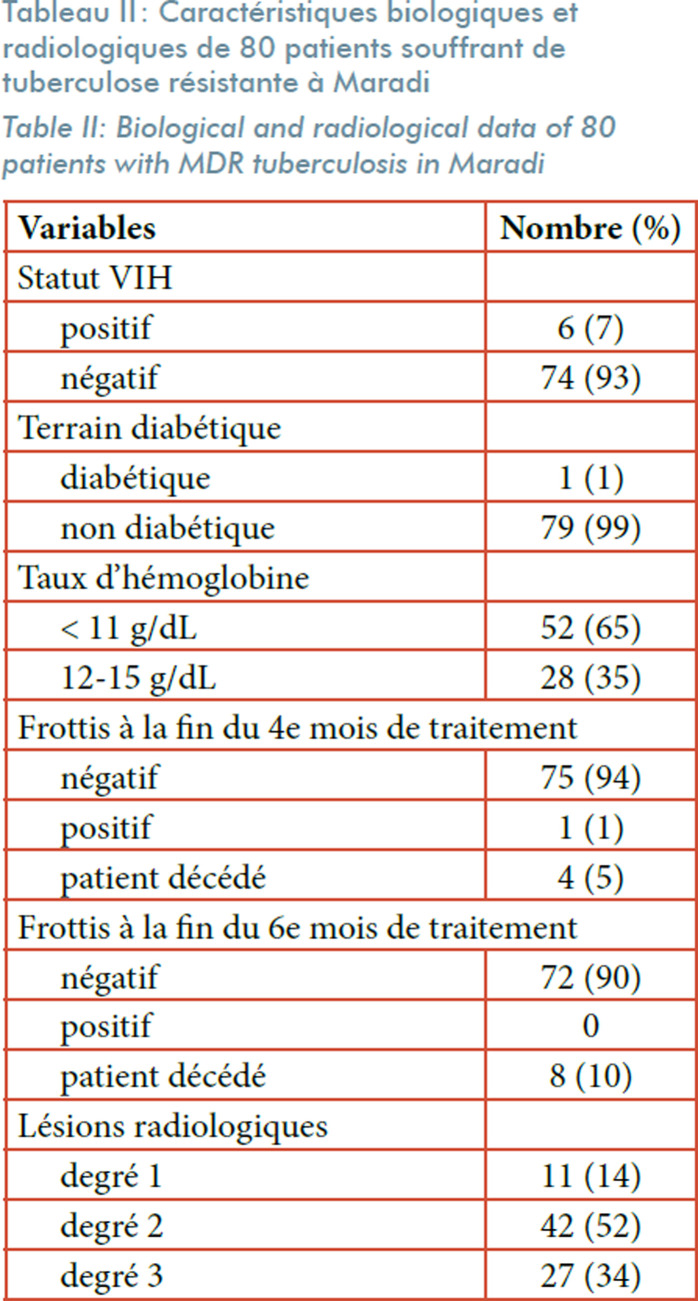
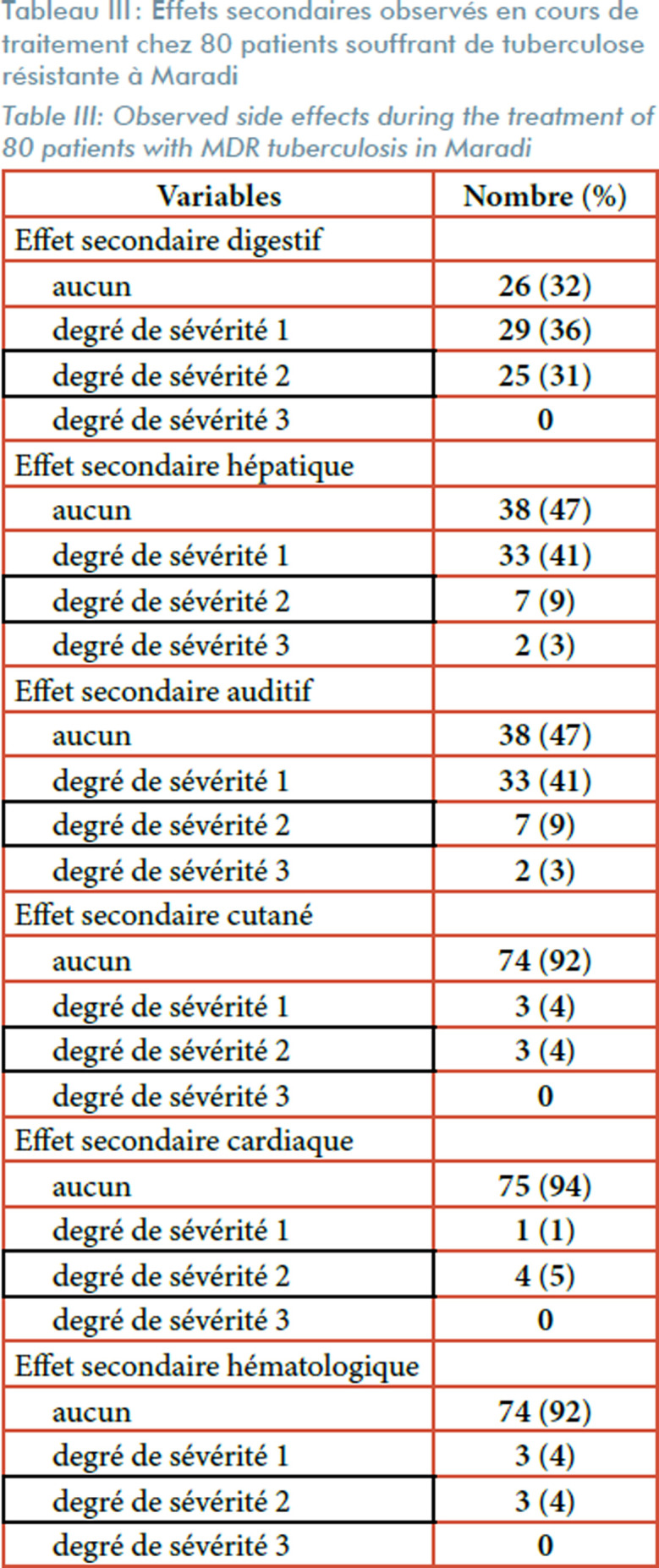
Results: A total of 80 patients were included in the present study (70 males and 10 females, mean age 34.4 years with extremes ranging from 18 to 71 years). Patients aged 18-35 years accounted for more than half. Patients with primary treatment failure were the most frequent type (36%) followed by patients with retreatment failure (24%) and patients with retreatment relapse (17%). It should be noted that 77 patients (96%) were previously treated for TB and only 3 patients (4%) were new cases. The majority of patients (70%) had a Body mass index of less than 18 kg/m2. 7.5% of patients were HIV positive, one was diabetic, 52% of the patients had grade 2 radiological lesions. Grade 1 deafness was noted at the beginning of treatment in 3%. A third of patients (36%) were primary treatment failures. The treatment protocol was as follows: 4KmMfxPtoCfzHZE/5MfxCfzZE. Only 1 patient had a positive culture at the end of the 4th month of treatment. Most of the patients had experienced adverse events, mainly digestive, with vomiting being the most common. The therapeutic success rate was 88%. We noted 10% of deaths, 1% of therapeutic failure and 1% of lost to follow-up.Six months after treatment, 48 patients (60%) were smear negative and 43 (54%) were culture negative. In 32 patients (40%), the smear was not performed and culture was not performed in 37.
Conclusion: The short treatment regime gives satisfactory results in the absence of resistance to fluoroquinolones, with rare adverse effects. In Niger, further efforts should be made to minimize the delay in diagnosis which is responsible for most deaths during treatment. A centre could usefully be designated to organize "TB consiliums" allowing any practitioner to submit difficult cases of MDR-TB.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


