Comparison of short-term outcomes of open and laparoscopic assisted pancreaticoduodenectomy for periampullary carcinoma: A propensity score-matched analysis.
{"title":"Comparison of short-term outcomes of open and laparoscopic assisted pancreaticoduodenectomy for periampullary carcinoma: A propensity score-matched analysis.","authors":"Utpal Anand, Rohith Kodali, Kunal Parasar, Basant Narayan Singh, Kislay Kant, Sitaram Yadav, Saad Anwar, Abhishek Arora","doi":"10.14701/ahbps.23-144","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Postoperative pancreatic fistula is the key worry in the ongoing debate about the safety and effectiveness of total laparoscopic pancreaticoduodenectomy (TLPD). Laparoscopic-assisted pancreaticoduodenectomy (LAPD), a hybrid approach combining laparoscopic resection and anastomosis with a small incision, is an alternative to TLPD. This study compares the short-term outcomes and oncological efficacy of LAPD vs. open pancreaticoduodenectomy (OPD).</p><p><strong>Methods: </strong>A retrospective analysis of data of all patients who underwent LAPD or OPD for periampullary carcinoma at a tertiary care center in Northeast India from July 2019 to August 2023 was done. A total of 30 LAPDs and 30 OPDs were compared after 1:1 propensity score matching. Demographic data, intraoperative and postoperative data (30 days), and pathological data were compared.</p><p><strong>Results: </strong>The study included a total of 93 patients, 30 underwent LAPD and 62 underwent OPD. After propensity score matching, the matched cohort included 30 patients in both groups. The LAPD presented several advantages over the OPD group, including a shorter incision length, reduced postoperative pain, earlier initiation of oral feeding, and shorter hospital stays. LAPD was not found to be inferior to OPD in terms of pancreatic fistula incidence (Grade B, 30.0% vs. 33.3%), achieving R0 resection (100% vs. 93.3%), and the number of lymph nodes harvested (12 vs. 14, <i>p</i> = 0.620). No significant differences in blood loss, short-term complications, pathological outcomes, readmissions, and early (30-day) mortality were observed between the two groups.</p><p><strong>Conclusions: </strong>LAPD has comparable safety, technical feasibility, and short-term oncological efficacy.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"220-228"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128788/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.23-144","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/22 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: Postoperative pancreatic fistula is the key worry in the ongoing debate about the safety and effectiveness of total laparoscopic pancreaticoduodenectomy (TLPD). Laparoscopic-assisted pancreaticoduodenectomy (LAPD), a hybrid approach combining laparoscopic resection and anastomosis with a small incision, is an alternative to TLPD. This study compares the short-term outcomes and oncological efficacy of LAPD vs. open pancreaticoduodenectomy (OPD).
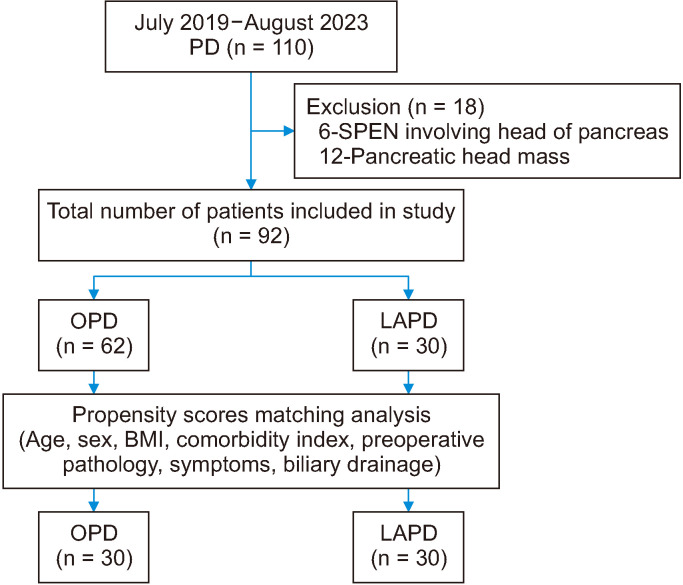
Methods: A retrospective analysis of data of all patients who underwent LAPD or OPD for periampullary carcinoma at a tertiary care center in Northeast India from July 2019 to August 2023 was done. A total of 30 LAPDs and 30 OPDs were compared after 1:1 propensity score matching. Demographic data, intraoperative and postoperative data (30 days), and pathological data were compared.
Results: The study included a total of 93 patients, 30 underwent LAPD and 62 underwent OPD. After propensity score matching, the matched cohort included 30 patients in both groups. The LAPD presented several advantages over the OPD group, including a shorter incision length, reduced postoperative pain, earlier initiation of oral feeding, and shorter hospital stays. LAPD was not found to be inferior to OPD in terms of pancreatic fistula incidence (Grade B, 30.0% vs. 33.3%), achieving R0 resection (100% vs. 93.3%), and the number of lymph nodes harvested (12 vs. 14, p = 0.620). No significant differences in blood loss, short-term complications, pathological outcomes, readmissions, and early (30-day) mortality were observed between the two groups.
Conclusions: LAPD has comparable safety, technical feasibility, and short-term oncological efficacy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


