Calvin X Geng, Anuragh R Gudur, Jagannath Kadiyala, Daniel S Strand, Vanessa M Shami, Andrew Y Wang, Alexander Podboy, Tri M Le, Matthew Reilley, Victor Zaydfudim, Ross C D Buerlein
{"title":"Associations between income and survival in cholangiocarcinoma: A comprehensive subtype-based analysis.","authors":"Calvin X Geng, Anuragh R Gudur, Jagannath Kadiyala, Daniel S Strand, Vanessa M Shami, Andrew Y Wang, Alexander Podboy, Tri M Le, Matthew Reilley, Victor Zaydfudim, Ross C D Buerlein","doi":"10.14701/ahbps.23-136","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Socioeconomic determinants of health are incompletely characterized in cholangiocarcinoma (CCA). We assessed how socioeconomic status influences initial treatment decisions and survival outcomes in patients with CCA, additionally performing multiple sub-analyses based on anatomic location of the primary tumor.</p><p><strong>Methods: </strong>Observational study using the 2018 submission of the Surveillance, Epidemiology, and End Results (SEER)-18 Database. In total, 5,476 patients from 2004-2015 with a CCA were separated based on median household income (MHI) into low income (< 25th percentile of MHI) and high income (> 25th percentile of MHI) groups. Seventy-three percent of patients had complete follow up data, and were included in survival analyses. Survival and treatment outcomes were calculated using R-studio.</p><p><strong>Results: </strong>When all cases of CCA were included, the high-income group was more likely than the low-income to receive surgery, chemotherapy, and local tumor destruction modalities. Initial treatment modality based on income differed significantly between tumor locations. Patients of lower income had higher overall and cancer-specific mortality at 2 and 5 years. Non-cancer mortality was similar between the groups. Survival differences identified in the overall cohort were maintained in the intrahepatic CCA subgroup. No differences between income groups were noted in cancer-specific or overall mortality for perihilar tumors, with variable differences in the distal cohort.</p><p><strong>Conclusions: </strong>Lower income was associated with higher rates of cancer-specific mortality and lower rates of surgical resection in CCA. There were significant differences in treatment selection and outcomes between intrahepatic, perihilar, and distal tumors. Population-based strategies aimed at identifying possible etiologies for these disparities are paramount to improving patient outcomes.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"144-154"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128791/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.23-136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/15 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: Socioeconomic determinants of health are incompletely characterized in cholangiocarcinoma (CCA). We assessed how socioeconomic status influences initial treatment decisions and survival outcomes in patients with CCA, additionally performing multiple sub-analyses based on anatomic location of the primary tumor.
Methods: Observational study using the 2018 submission of the Surveillance, Epidemiology, and End Results (SEER)-18 Database. In total, 5,476 patients from 2004-2015 with a CCA were separated based on median household income (MHI) into low income (< 25th percentile of MHI) and high income (> 25th percentile of MHI) groups. Seventy-three percent of patients had complete follow up data, and were included in survival analyses. Survival and treatment outcomes were calculated using R-studio.
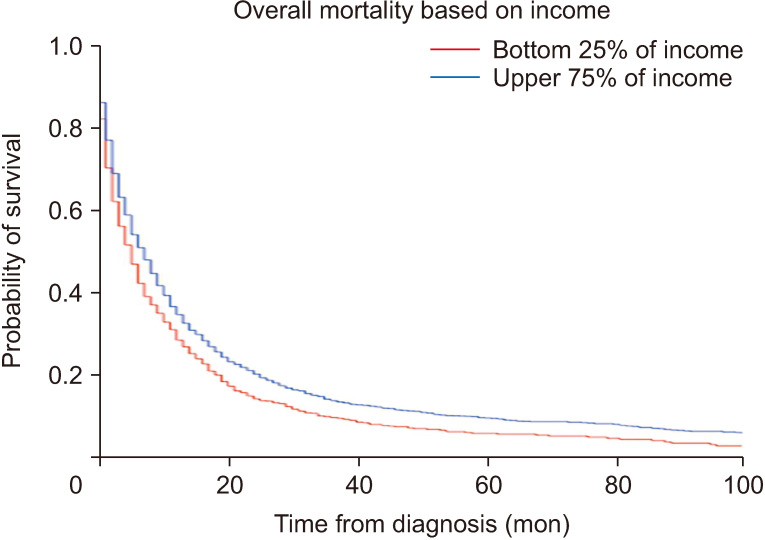
Results: When all cases of CCA were included, the high-income group was more likely than the low-income to receive surgery, chemotherapy, and local tumor destruction modalities. Initial treatment modality based on income differed significantly between tumor locations. Patients of lower income had higher overall and cancer-specific mortality at 2 and 5 years. Non-cancer mortality was similar between the groups. Survival differences identified in the overall cohort were maintained in the intrahepatic CCA subgroup. No differences between income groups were noted in cancer-specific or overall mortality for perihilar tumors, with variable differences in the distal cohort.
Conclusions: Lower income was associated with higher rates of cancer-specific mortality and lower rates of surgical resection in CCA. There were significant differences in treatment selection and outcomes between intrahepatic, perihilar, and distal tumors. Population-based strategies aimed at identifying possible etiologies for these disparities are paramount to improving patient outcomes.
背景/目的:胆管癌(CCA)患者健康的社会经济决定因素尚未完全定性。我们评估了社会经济状况如何影响 CCA 患者的初始治疗决策和生存结果,此外还根据原发肿瘤的解剖位置进行了多项子分析:使用 2018 年提交的监测、流行病学和最终结果(SEER)-18 数据库进行观察研究。根据家庭收入中位数(MHI)将2004-2015年的5476名CCA患者分为低收入组(MHI第25百分位数)。73%的患者拥有完整的随访数据,并被纳入生存分析。生存率和治疗结果使用 R-studio 进行计算:结果表明:当纳入所有 CCA 病例时,高收入组比低收入组更有可能接受手术、化疗和局部肿瘤切除术。基于收入的初始治疗方式在不同肿瘤位置之间存在显著差异。收入较低的患者在2年和5年内的总死亡率和癌症特异性死亡率较高。各组的非癌症死亡率相似。在肝内 CCA 亚组中,总体队列中发现的生存率差异依然存在。在肝周肿瘤的癌症特异性死亡率或总死亡率方面,各收入组之间没有发现差异,远端队列中的差异则不尽相同:结论:较低的收入与较高的癌症特异性死亡率和较低的CCA手术切除率有关。肝内肿瘤、肝周肿瘤和远端肿瘤在治疗选择和治疗效果方面存在明显差异。要改善患者的预后,必须采取基于人群的策略,找出造成这些差异的可能病因。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


