Impact of the combination of abdominal peripheral nerve block and neuromuscular blockade on the surgical space during robot-assisted laparoscopic surgery: a prospective randomized controlled study.
{"title":"Impact of the combination of abdominal peripheral nerve block and neuromuscular blockade on the surgical space during robot-assisted laparoscopic surgery: a prospective randomized controlled study.","authors":"Satoko Noguchi, Junichi Saito, Kishiko Nakai, Masato Kitayama, Kazuyoshi Hirota","doi":"10.1007/s00540-024-03309-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The impact of the combination of abdominal peripheral nerve block (PNB) and the depth of neuromuscular blockade on the surgical field were assessed.</p><p><strong>Methods: </strong>Thirty-eight patients undergoing elective robot-assisted laparoscopic radical prostatectomy (RARP) were randomized into two groups: a PNB group (moderate neuromuscular block [train-of-four 1-3 twitches] with abdominal PNB) and a non-PNB group (deep neuromuscular block [post-tetanic count 0-2 twitches] without abdominal PNB). The primary outcome was the change in the depth of the abdominal cavity relaxation assessed by the change in the distance (Δdistance) between the umbilicus port and peritoneum upon pneumoperitoneal pressure increase from 8 to 12 mmHg. The secondary outcomes were the CO<sub>2</sub> usage for the pneumoperitoneal pressure increase and the subjective differences in the Surgical Rating Score (SRS) during surgery.</p><p><strong>Results: </strong>The Δdistance and the CO<sub>2</sub> usage from 8 to 12 mmHg did not differ significantly between the non-PNB and PNB groups (1.34 ± 0.65 vs. 1.28 ± 0.61 cm, p = 0.763 and 3.64 ± 1.68 vs. 4.34 ± 1.44 L, p = 0.180, respectively). There was also no significant difference in SRS. Comparisons of the Δdistance values for pressure increases from 6 to 8 mmHg, 6 to 10 mmHg and 6 to 12 mmHg between the non-PNB and PNB groups also showed no between-group differences, despite significant intra-group differences (p < 0.001) by pressure increment.</p><p><strong>Conclusions: </strong>Our findings indicate that moderate neuromuscular block with abdominal PNB maintained an adequate surgical space for RARP, with no significant difference from the space achieved by deep neuromuscular block.</p>","PeriodicalId":14997,"journal":{"name":"Journal of Anesthesia","volume":null,"pages":null},"PeriodicalIF":2.8000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00540-024-03309-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The impact of the combination of abdominal peripheral nerve block (PNB) and the depth of neuromuscular blockade on the surgical field were assessed.
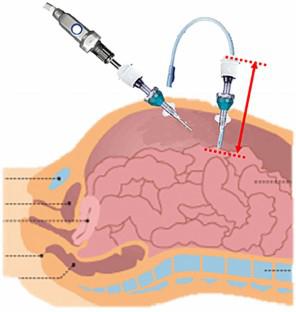
Methods: Thirty-eight patients undergoing elective robot-assisted laparoscopic radical prostatectomy (RARP) were randomized into two groups: a PNB group (moderate neuromuscular block [train-of-four 1-3 twitches] with abdominal PNB) and a non-PNB group (deep neuromuscular block [post-tetanic count 0-2 twitches] without abdominal PNB). The primary outcome was the change in the depth of the abdominal cavity relaxation assessed by the change in the distance (Δdistance) between the umbilicus port and peritoneum upon pneumoperitoneal pressure increase from 8 to 12 mmHg. The secondary outcomes were the CO2 usage for the pneumoperitoneal pressure increase and the subjective differences in the Surgical Rating Score (SRS) during surgery.
Results: The Δdistance and the CO2 usage from 8 to 12 mmHg did not differ significantly between the non-PNB and PNB groups (1.34 ± 0.65 vs. 1.28 ± 0.61 cm, p = 0.763 and 3.64 ± 1.68 vs. 4.34 ± 1.44 L, p = 0.180, respectively). There was also no significant difference in SRS. Comparisons of the Δdistance values for pressure increases from 6 to 8 mmHg, 6 to 10 mmHg and 6 to 12 mmHg between the non-PNB and PNB groups also showed no between-group differences, despite significant intra-group differences (p < 0.001) by pressure increment.
Conclusions: Our findings indicate that moderate neuromuscular block with abdominal PNB maintained an adequate surgical space for RARP, with no significant difference from the space achieved by deep neuromuscular block.
期刊介绍:
The Journal of Anesthesia is the official journal of the Japanese Society of Anesthesiologists. This journal publishes original articles, review articles, special articles, clinical reports, short communications, letters to the editor, and book and multimedia reviews. The editors welcome the submission of manuscripts devoted to anesthesia and related topics from any country of the world. Membership in the Society is not a prerequisite.
The Journal of Anesthesia (JA) welcomes case reports that show unique cases in perioperative medicine, intensive care, emergency medicine, and pain management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


