Nathan Hearn, Alexandria Leppien, Patrick O'Connor, Katelyn Cahill, Daisy Atwell, Dinesh Vignarajah, Myo Min
{"title":"Radiotherapy dose escalation using pre-treatment diffusion-weighted imaging in locally advanced rectal cancer: a planning study.","authors":"Nathan Hearn, Alexandria Leppien, Patrick O'Connor, Katelyn Cahill, Daisy Atwell, Dinesh Vignarajah, Myo Min","doi":"10.1093/bjro/tzad001","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Diffusion-weighted MRI (DWI) may provide biologically relevant target volumes for dose-escalated radiotherapy in locally advanced rectal cancer (LARC). This planning study assessed the dosimetric feasibility of delivering hypofractionated boost treatment to intra-tumoural regions of restricted diffusion prior to conventional long-course radiotherapy.</p><p><strong>Methods: </strong>Ten patients previously treated with curative-intent standard long-course radiotherapy (50 Gy/25#) were re-planned. Boost target volumes (<i>BTVs</i>) were delineated semi-automatically using 40th centile intra-tumoural apparent diffusion coefficient value with expansions (anteroposterior 11 mm, transverse 7 mm, craniocaudal 13 mm). Biased-dosed combined plans consisted of a single-fraction volumetric modulated arc therapy flattening-filter-free (VMAT-FFF) boost (phase 1) of 5, 7, or 10 Gy before long-course VMAT (phase 2). Phase 1 plans were assessed with reference to stereotactic conformality and deliverability measures. Combined plans were evaluated with reference to standard long-course therapy dose constraints.</p><p><strong>Results: </strong>Phase 1 BTV dose targets at 5/7/10 Gy were met in all instances. Conformality constraints were met with only 1 minor violation at 5 and 7 Gy. All phase 1 and combined phase 1 + 2 plans passed patient-specific quality assurance. Combined phase 1 + 2 plans generally met organ-at-risk dose constraints. Exceptions included high-dose spillage to bladder and large bowel, predominantly in cases where previously administered, clinically acceptable non-boosted plans also could not meet constraints.</p><p><strong>Conclusions: </strong>Targeted upfront LARC radiotherapy dose escalation to DWI-defined is feasible with appropriate patient selection and preparation.</p><p><strong>Advances in knowledge: </strong>This is the first study to evaluate the feasibility of DWI-targeted upfront radiotherapy boost in LARC. This work will inform an upcoming clinical feasibility study.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"6 1","pages":"tzad001"},"PeriodicalIF":2.1000,"publicationDate":"2023-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10860507/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjro/tzad001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
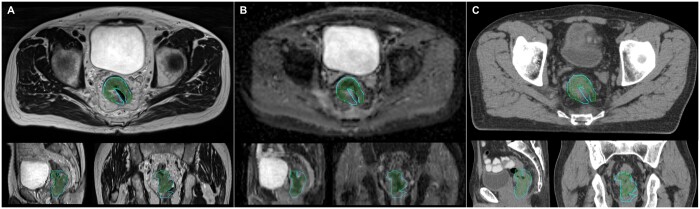
Objectives: Diffusion-weighted MRI (DWI) may provide biologically relevant target volumes for dose-escalated radiotherapy in locally advanced rectal cancer (LARC). This planning study assessed the dosimetric feasibility of delivering hypofractionated boost treatment to intra-tumoural regions of restricted diffusion prior to conventional long-course radiotherapy.
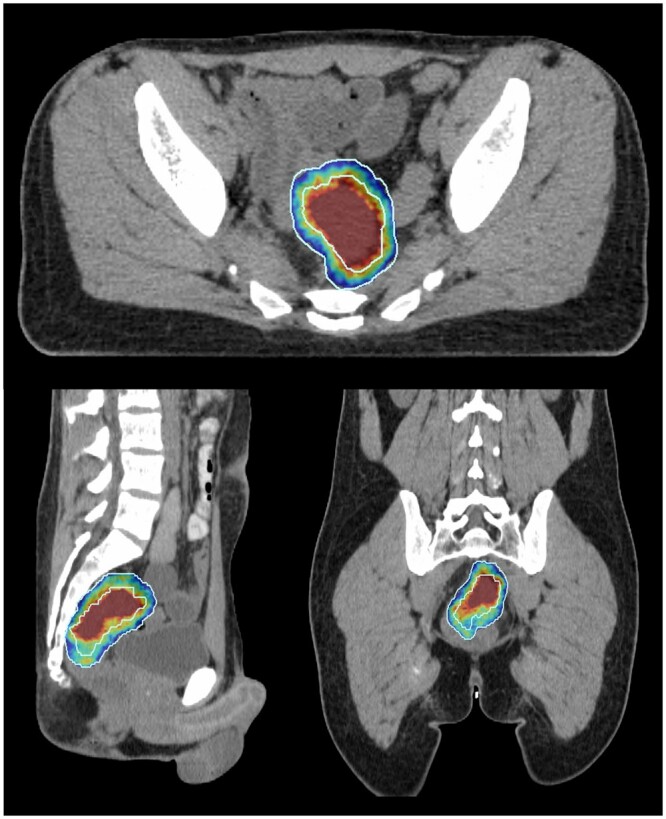
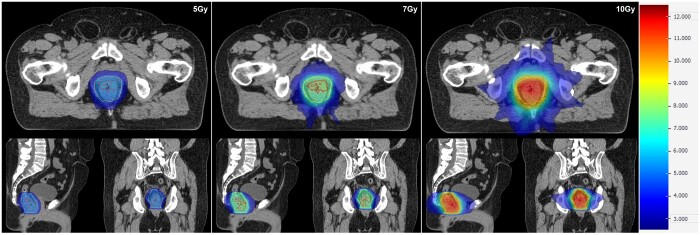
Methods: Ten patients previously treated with curative-intent standard long-course radiotherapy (50 Gy/25#) were re-planned. Boost target volumes (BTVs) were delineated semi-automatically using 40th centile intra-tumoural apparent diffusion coefficient value with expansions (anteroposterior 11 mm, transverse 7 mm, craniocaudal 13 mm). Biased-dosed combined plans consisted of a single-fraction volumetric modulated arc therapy flattening-filter-free (VMAT-FFF) boost (phase 1) of 5, 7, or 10 Gy before long-course VMAT (phase 2). Phase 1 plans were assessed with reference to stereotactic conformality and deliverability measures. Combined plans were evaluated with reference to standard long-course therapy dose constraints.
Results: Phase 1 BTV dose targets at 5/7/10 Gy were met in all instances. Conformality constraints were met with only 1 minor violation at 5 and 7 Gy. All phase 1 and combined phase 1 + 2 plans passed patient-specific quality assurance. Combined phase 1 + 2 plans generally met organ-at-risk dose constraints. Exceptions included high-dose spillage to bladder and large bowel, predominantly in cases where previously administered, clinically acceptable non-boosted plans also could not meet constraints.
Conclusions: Targeted upfront LARC radiotherapy dose escalation to DWI-defined is feasible with appropriate patient selection and preparation.
Advances in knowledge: This is the first study to evaluate the feasibility of DWI-targeted upfront radiotherapy boost in LARC. This work will inform an upcoming clinical feasibility study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


