Evelyn Waugh, Juan Glinka, Daniel Breadner, Rachel Liu, Ephraim Tang, Laura Allen, Stephen Welch, Ken Leslie, Anton Skaro
{"title":"Survival benefit of neoadjuvant FOLFIRINOX for patients with borderline resectable pancreatic cancer.","authors":"Evelyn Waugh, Juan Glinka, Daniel Breadner, Rachel Liu, Ephraim Tang, Laura Allen, Stephen Welch, Ken Leslie, Anton Skaro","doi":"10.14701/ahbps.23-107","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>While patients with borderline resectable pancreatic cancer (BRPC) are a target population for neoadjuvant chemotherapy (NAC), formal guidelines for neoadjuvant therapy are lacking. We assessed the perioperative and oncological outcomes in patients with BRPC undergoing NAC with FOLFIRINOX for patients undergoing upfront surgery (US).</p><p><strong>Methods: </strong>The AHPBA criteria for borderline resectability and/or a CA19-9 level > 100 μ/mL defined borderline resectable tumors retrieved from a prospectively populated institutional registry from 2007 to 2020. The primary outcome was overall survival (OS) at 1 and 3 years. A Cox Proportional Hazard model based on intention to treat was used. A receiver-operator characteristics (ROC) curve was constructed to assess the discriminatory capability of the use of CA19-9 > 100 μ/mL to predict resectability and mortality.</p><p><strong>Results: </strong>Forty BRPC patients underwent NAC, while 46 underwent US. The median OS with NAC was 19.8 months (interquartile range [IQR], 10.3-44.24) vs. 10.6 months (IQR, 6.37-17.6) with US. At 1 year, 70% of the NAC group and 41.3% of the US group survived (<i>p</i> = 0.008). At 3 years, 42.5 % of the NAC group and 10.9% of the US group survived (<i>p</i> = 0.001). NAC significantly reduced the hazard of death (adjusted hazard ratio, 0.20; 95% confidence interval, 0.07-0.54; <i>p</i> = 0.001). CA19-9 > 100 μ/mL showed poor discrimination in predicting mortality, but was a moderate predictor of resectability.</p><p><strong>Conclusions: </strong>We found a survival benefit of NAC with FOLFIRINOX for BRPC. Greater pre-treatment of CA19-9 and multivessel involvement on initial imaging were associated with progression of the disease following NAC.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"229-237"},"PeriodicalIF":1.7000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11128787/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.23-107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/1 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: While patients with borderline resectable pancreatic cancer (BRPC) are a target population for neoadjuvant chemotherapy (NAC), formal guidelines for neoadjuvant therapy are lacking. We assessed the perioperative and oncological outcomes in patients with BRPC undergoing NAC with FOLFIRINOX for patients undergoing upfront surgery (US).
Methods: The AHPBA criteria for borderline resectability and/or a CA19-9 level > 100 μ/mL defined borderline resectable tumors retrieved from a prospectively populated institutional registry from 2007 to 2020. The primary outcome was overall survival (OS) at 1 and 3 years. A Cox Proportional Hazard model based on intention to treat was used. A receiver-operator characteristics (ROC) curve was constructed to assess the discriminatory capability of the use of CA19-9 > 100 μ/mL to predict resectability and mortality.
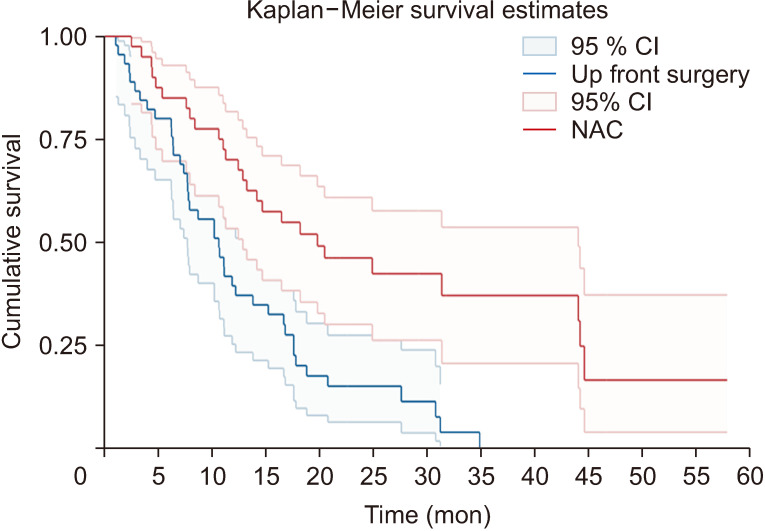
Results: Forty BRPC patients underwent NAC, while 46 underwent US. The median OS with NAC was 19.8 months (interquartile range [IQR], 10.3-44.24) vs. 10.6 months (IQR, 6.37-17.6) with US. At 1 year, 70% of the NAC group and 41.3% of the US group survived (p = 0.008). At 3 years, 42.5 % of the NAC group and 10.9% of the US group survived (p = 0.001). NAC significantly reduced the hazard of death (adjusted hazard ratio, 0.20; 95% confidence interval, 0.07-0.54; p = 0.001). CA19-9 > 100 μ/mL showed poor discrimination in predicting mortality, but was a moderate predictor of resectability.
Conclusions: We found a survival benefit of NAC with FOLFIRINOX for BRPC. Greater pre-treatment of CA19-9 and multivessel involvement on initial imaging were associated with progression of the disease following NAC.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


