Sudipta Chattopadhyay, Felicia Adjei, Attila Kardos
{"title":"Changes in Cardiac Electrical Biomarker in Response to Coronary Arterial Occlusion: An Experimental Observation.","authors":"Sudipta Chattopadhyay, Felicia Adjei, Attila Kardos","doi":"10.1007/s12265-024-10487-w","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiac electrical biomarker (CEB), an indicator of ischaemia-induced change in myocyte polarity, has been proposed for diagnosis of acute coronary syndrome. However, effect of coronary occlusion on CEB has not been demonstrated. CEB was acquired before (CEB0), during maximal adenosine hyperaemia (CEBhyp), balloon inflations (CEBmax) and 1 (CEB1h), 2 (CEB2h) and 3 (CEB3h) h after percutaneous coronary intervention along with pre- and post-procedural troponin-I. CEB of subjects with non-cardiac chest pain without risk factors was used as controls (CEBc). \"Late recovery\" (LR) of CEB was defined as CEB3h > median-CEB0. CEB was recorded in 75 patients undergoing stenting (group 1) including 8 with FFR < 0.8 (group 1a), 25 with FFR ≥ 0.8 (group 2) and 49 controls. In group 1, CEB0 (median, IQR) was higher than CEBc (48.0; 29.5-88.3 vs 30.0; 17.0-44.0; p < 0.001). CEBmax (185; 105.0-331.0) was higher than CEB0 (p < 0.0001). CEB1h (78.0; 31.5-143.8; p < 0.0001) and CEB2h (63.0; 31.5-114.3; p = 0.039) were higher than CEB0 while CEB3h (54.0; 24.3-94.8, p = 0.152) was similar. LR occurred in 50.7% patients. CEBmax predicted LR (OR 1.01, 95% CI 1.00-1.01, p < 0.001) (AUC 0.759, p < 0.001). CEB0 in group 1a and group 2 were similar (p = 0.524). CEBhyp was higher than CEB0 in group 1a (126.0, 109.5-266.0 vs 47.5, 20.5-73.5; p = 0.016) and group 2 (44.0, 27.8-104.8 vs 39.0, 24.0-90.3; p = 0.014). CEBhyp was higher in group 1a than 2 (p = 0.039). CEBhyp (AUC 0.75, p = 0.017) accurately predicted FFR < 0.8. Coronary arterial occlusion increases CEB that retains a \"memory\" of the ischaemic event. CEBhyp was higher only when FFR was ischaemic and accurately identified FFR < 0.8.</p>","PeriodicalId":15224,"journal":{"name":"Journal of Cardiovascular Translational Research","volume":" ","pages":"870-878"},"PeriodicalIF":2.4000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Translational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12265-024-10487-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
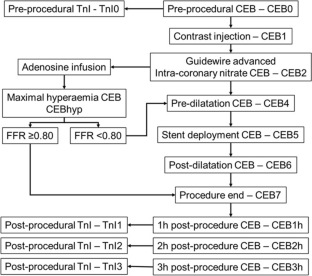
Cardiac electrical biomarker (CEB), an indicator of ischaemia-induced change in myocyte polarity, has been proposed for diagnosis of acute coronary syndrome. However, effect of coronary occlusion on CEB has not been demonstrated. CEB was acquired before (CEB0), during maximal adenosine hyperaemia (CEBhyp), balloon inflations (CEBmax) and 1 (CEB1h), 2 (CEB2h) and 3 (CEB3h) h after percutaneous coronary intervention along with pre- and post-procedural troponin-I. CEB of subjects with non-cardiac chest pain without risk factors was used as controls (CEBc). "Late recovery" (LR) of CEB was defined as CEB3h > median-CEB0. CEB was recorded in 75 patients undergoing stenting (group 1) including 8 with FFR < 0.8 (group 1a), 25 with FFR ≥ 0.8 (group 2) and 49 controls. In group 1, CEB0 (median, IQR) was higher than CEBc (48.0; 29.5-88.3 vs 30.0; 17.0-44.0; p < 0.001). CEBmax (185; 105.0-331.0) was higher than CEB0 (p < 0.0001). CEB1h (78.0; 31.5-143.8; p < 0.0001) and CEB2h (63.0; 31.5-114.3; p = 0.039) were higher than CEB0 while CEB3h (54.0; 24.3-94.8, p = 0.152) was similar. LR occurred in 50.7% patients. CEBmax predicted LR (OR 1.01, 95% CI 1.00-1.01, p < 0.001) (AUC 0.759, p < 0.001). CEB0 in group 1a and group 2 were similar (p = 0.524). CEBhyp was higher than CEB0 in group 1a (126.0, 109.5-266.0 vs 47.5, 20.5-73.5; p = 0.016) and group 2 (44.0, 27.8-104.8 vs 39.0, 24.0-90.3; p = 0.014). CEBhyp was higher in group 1a than 2 (p = 0.039). CEBhyp (AUC 0.75, p = 0.017) accurately predicted FFR < 0.8. Coronary arterial occlusion increases CEB that retains a "memory" of the ischaemic event. CEBhyp was higher only when FFR was ischaemic and accurately identified FFR < 0.8.
期刊介绍:
Journal of Cardiovascular Translational Research (JCTR) is a premier journal in cardiovascular translational research.
JCTR is the journal of choice for authors seeking the broadest audience for emerging technologies, therapies and diagnostics, pre-clinical research, and first-in-man clinical trials.
JCTR''s intent is to provide a forum for critical evaluation of the novel cardiovascular science, to showcase important and clinically relevant aspects of the new research, as well as to discuss the impediments that may need to be overcome during the translation to patient care.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


