{"title":"A novel strategy for treating oncogene-mutated tumors by targeting tumor microenvironment and synergistically enhancing anti-PD-1 immunotherapy","authors":"Yingqiang Liu, Linjiang Tong, Mengge Zhang, Qi Zhang, Qiupei Liu, Fang Feng, Yan Li, Mengzhen Lai, Haotian Tang, Yi Chen, Meiyu Geng, Wenhu Duan, Jian Ding, Hua Xie","doi":"10.1002/cac2.12521","DOIUrl":null,"url":null,"abstract":"<p>Oncogenes are critical factors in tumorigenesis of diverse cancer types and play essential roles in tumor immune escape. Mutations in Kirsten rat sarcoma viral oncogene homolog (<i>KRAS</i>) and epidermal growth factor receptor (<i>EGFR</i>) are among the most frequent gain-of-function alterations [<span>1</span>]. After many years of in-depth research, inhibitors targeting <i>EGFR</i> or <i>KRAS</i> mutations have been successfully developed, however, their clinical benefit is relatively limited, and they will inevitably encounter the challenge of drug resistance. The emergence of resistance is attributed to secondary mutations in driver genes and other complicated factors. It is worth noting that approved treatment strategies are currently lacking for tumors with different types of <i>KRAS</i> or <i>EGFR</i> mutations, including <i>KRAS<sup>G12D</sup></i>, <i>KRAS<sup>G13D</sup></i>, and <i>EGFR<sup>C797S</sup></i> mutations that are common in tumors [<span>2</span>]. Additionally, oncogene mutations could trigger a cascade of tumor microenvironment changes, ultimately resulting in tumor progression or resistance to programmed death-1 (PD-1) antibody therapy [<span>3, 4</span>]. SYHA1813, a novel vascular endothelial growth factor receptor (VEGFR) and colony-stimulating factor 1 receptor (CSF1R) dual inhibitor, exhibited potent preclinical anti-glioma activity by inhibiting angiogenesis and promoting tumor immunity and showed promising efficacy in an ongoing clinical study (ChiCTR2100045380) [<span>5, 6</span>]. Here, we determined SYHA1813's antitumor activity in tumor models bearing <i>KRAS</i> or <i>EGFR</i> mutations.</p><p>We first examined the effects of SYHA1813 against cell line-derived xenograft (CDX) tumor models containing <i>KRAS<sup>G12C</sup></i> mutation (NCI-H358 lung cancer), <i>KRAS<sup>G12D</sup></i> mutation (PANC-1 pancreatic cancer) and wild-type <i>KRAS</i> (<i>KRAS<sup>WT</sup></i>) (HT-29 colorectal cancer). The results demonstrated that oral administration of SYHA1813 at a dose of 10 mg/kg significantly reduced tumor growth in the NCI-H358 xenograft model, with comparable efficacy to the US Food and Drug Administration (FDA) approved KRAS<sup>G12C</sup> inhibitor sotorasib (AMG510) (Figure 1A). SYHA1813 treatment also resulted in tumor regression in PANC-1 and HT-29 xenograft models (Figure 1B-C). No significant body weight loss was observed in all groups (Supplementary Figure S1). Moreover, considering the emergence of drug resistance as a significant challenge of AMG510, we established a drug resistance model of AMG510 (designated as AMG510R). We found that although AMG510 exhibited attenuated efficacy against the AMG510R model compared to the NCI-H358 model, SYHA1813 could still suppress the growth of drug-resistant tumors at the same dose (Figure 1D). Furthermore, SYHA1813 was evaluated in two patient-derived xenograft (PDX) models, including gastric tumor model GC-1-005 (<i>KRAS<sup>G13D</sup></i>) and colorectal tumor model CRC-1-003 (<i>KRAS<sup>WT</sup></i>) (Figure 1E). SYHA1813 also exhibited potent antitumor activity in these PDX models (Figure 1F-G). Given that SYHA1813 exerted antitumor effects by modulating angiogenesis and macrophages, we further analyzed the expression of the markers associated with angiogenesis, macrophages, and proliferation in NCI-H358 and HT-29 tumor tissues. The immunohistochemistry (IHC) results showed that SYHA1813 significantly reduced the expression of angiogenic marker CD31, macrophage marker F4/80, M2-phenotype macrophage marker CD206 and arginase-1 (ARG1), and the tumor proliferation marker Ki67 (Figure 1H and Supplementary Figure S2). In summary, SYHA1813 exhibited robust antitumor activities across a panel of genetically and histologically heterogeneous <i>KRAS</i>-mutated tumor models, including the model resistant to AMG510.</p><p>We then asked whether SYHA1813 could suppress the growth of tumors carrying <i>EGFR</i> mutations or resistant to EGFR tyrosine kinase inhibitors (TKIs). To address this question, we initially employed the NCI-H1975 model containing <i>EGFR<sup>L858R/T790M</sup></i> mutation, which is resistant to the first-generation EGFR TKIs, and found that SYHA1813 significantly suppressed the tumor growth (Figure 1I). Then, we evaluated the activity of SYHA1813 against the tumor model carrying <i>EGFR<sup>C797S</sup></i> triple mutation (PC-9-OR) that is resistant to third-generation EGFR TKIs [<span>7</span>]. As shown in Figure 1J, osimertinib (AZD9291), the first FDA approved third-generation EGFR TKI, failed to inhibit tumor growth even at the dose of 10 mg/kg. However, we observed a significant deceleration with SYHA1813 in tumor growth rate at doses of 5 and 10 mg/kg (Figure 1J). Furthermore, we employed the osimertinib-resistant tumor (designated as AZDR) [<span>8</span>] and also observed significant suppression upon SYHA1813 monotherapy (Figure 1K). Similarly, in another resistant model (designated as 67R) to the third-generation EGFR TKI ASK120067 [<span>8</span>], SYHA1813 monotherapy inhibited tumor growth (Figure 1L). The IHC results also demonstrated a reduction in angiogenic and macrophage markers in tumor tissues following SYHA1813 administration (Supplementary Figure S3). These findings demonstrated that SYHA1813 exhibited potent antitumor activity in different EGFR TKI-resistant models.</p><p>Given that the response rates to immunotherapy are quite limited across most tumor types, including those carrying <i>KRAS</i> mutations, and importantly, angiogenesis and macrophages have been identified as key factors involved in the resistance to immunotherapy [<span>9</span>], we then validated whether SYHA1813 could enhance the antitumor activity of anti-PD-1 therapy in immunocompetent mice models bearing CT26 (<i>KRAS<sup>G12D</sup></i> mutation) and MC38 (<i>KRAS<sup>WT</sup></i>) colon cancer (Figure 1M-N). In both models, monotherapy with anti-PD-1 antibody or SYHA1813 yielded moderate to marked suppression of tumor growth, while the combination of SYHA1813 and anti-PD-1 antibody conferred significant advantages over each monotherapy group. In the CT26 and MC38 models, the combinational ratio was 1.88 and 1.42, respectively, both exceeding 1, indicative of a synergistic effect (Supplementary Table S1). Flow cytometry analysis revealed that the combination therapy significantly reduced F4/80<sup>+</sup> and CD206<sup>+</sup> macrophages (Figure 1O). Additionally, a noticeable increase of CD8<sup>+</sup> T cells was observed in the combination treatment group, along with an upregulation of granzyme B expression (Figure 1P), indicating an enhanced cytotoxic response against tumor cells.</p><p>Our study discovered the activities of SYHA1813 in <i>KRAS</i>- or <i>EGFR</i>-mutated tumors, providing support for further investigation of SYHA1813. Given potential variations in the response of subcutaneous tumors and other tumor types to angiogenic agents, further experiments in orthotopic models will be conducted. The findings in the current work highlight the feasibility of a therapeutic strategy targeting the tumor microenvironment, which can be applied to treat oncogene-driven cancers and overcome the challenge of drug resistance to targeted therapy.</p><p>Hua Xie, Jian Ding, Wenhu Duan, and Meiyu Geng supervised the project. Yingqiang Liu, Linjiang Tong, Mengge Zhang, Mengzhen Lai, Fang Feng, Haotian Tang, Yi Chen, and Yan Li conducted the experiments. Yingqiang Liu, Mengge Zhang, Qi Zhang and Qiupei Liu analyzed the data. Yingqiang Liu, Qiupei Liu, Hua Xie, Jian Ding, and Wenhu Duan wrote the manuscript.</p><p>The authors declare no potential conflicts of interest.</p><p>This research was supported by grants from the Natural Science Foundation of China for Innovation Research Group (81821005), the National Natural Science Foundation of China (82273948, 81573271 and 81903638), High-level Innovative Research Institute (2021B0909050003), State Key Laboratory of Drug Research (SKLDR-2023-TT-01 and SIMM2205KF-09), Lingang Laboratory (LG202103-02-02), and Institutes for Drug Discovery and Development, Chinese Academy of Sciences (CASIMM0120225003-1 and -2).</p><p>Animal experiments containing cell line-derived xenografts and patient-derived xenografts were carried out in accordance with the Guide for the Care and Use of Laboratory Animals and approved by the Institutional Animal Care and Use Committee of Shanghai Institute of Materia Medica (approval number 2021-04-DJ-59).</p><p>Not applicable.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 3","pages":"438-442"},"PeriodicalIF":20.1000,"publicationDate":"2024-02-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12521","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12521","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Oncogenes are critical factors in tumorigenesis of diverse cancer types and play essential roles in tumor immune escape. Mutations in Kirsten rat sarcoma viral oncogene homolog (KRAS) and epidermal growth factor receptor (EGFR) are among the most frequent gain-of-function alterations [1]. After many years of in-depth research, inhibitors targeting EGFR or KRAS mutations have been successfully developed, however, their clinical benefit is relatively limited, and they will inevitably encounter the challenge of drug resistance. The emergence of resistance is attributed to secondary mutations in driver genes and other complicated factors. It is worth noting that approved treatment strategies are currently lacking for tumors with different types of KRAS or EGFR mutations, including KRASG12D, KRASG13D, and EGFRC797S mutations that are common in tumors [2]. Additionally, oncogene mutations could trigger a cascade of tumor microenvironment changes, ultimately resulting in tumor progression or resistance to programmed death-1 (PD-1) antibody therapy [3, 4]. SYHA1813, a novel vascular endothelial growth factor receptor (VEGFR) and colony-stimulating factor 1 receptor (CSF1R) dual inhibitor, exhibited potent preclinical anti-glioma activity by inhibiting angiogenesis and promoting tumor immunity and showed promising efficacy in an ongoing clinical study (ChiCTR2100045380) [5, 6]. Here, we determined SYHA1813's antitumor activity in tumor models bearing KRAS or EGFR mutations.
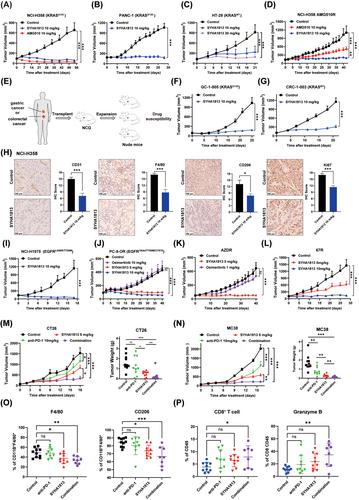
We first examined the effects of SYHA1813 against cell line-derived xenograft (CDX) tumor models containing KRASG12C mutation (NCI-H358 lung cancer), KRASG12D mutation (PANC-1 pancreatic cancer) and wild-type KRAS (KRASWT) (HT-29 colorectal cancer). The results demonstrated that oral administration of SYHA1813 at a dose of 10 mg/kg significantly reduced tumor growth in the NCI-H358 xenograft model, with comparable efficacy to the US Food and Drug Administration (FDA) approved KRASG12C inhibitor sotorasib (AMG510) (Figure 1A). SYHA1813 treatment also resulted in tumor regression in PANC-1 and HT-29 xenograft models (Figure 1B-C). No significant body weight loss was observed in all groups (Supplementary Figure S1). Moreover, considering the emergence of drug resistance as a significant challenge of AMG510, we established a drug resistance model of AMG510 (designated as AMG510R). We found that although AMG510 exhibited attenuated efficacy against the AMG510R model compared to the NCI-H358 model, SYHA1813 could still suppress the growth of drug-resistant tumors at the same dose (Figure 1D). Furthermore, SYHA1813 was evaluated in two patient-derived xenograft (PDX) models, including gastric tumor model GC-1-005 (KRASG13D) and colorectal tumor model CRC-1-003 (KRASWT) (Figure 1E). SYHA1813 also exhibited potent antitumor activity in these PDX models (Figure 1F-G). Given that SYHA1813 exerted antitumor effects by modulating angiogenesis and macrophages, we further analyzed the expression of the markers associated with angiogenesis, macrophages, and proliferation in NCI-H358 and HT-29 tumor tissues. The immunohistochemistry (IHC) results showed that SYHA1813 significantly reduced the expression of angiogenic marker CD31, macrophage marker F4/80, M2-phenotype macrophage marker CD206 and arginase-1 (ARG1), and the tumor proliferation marker Ki67 (Figure 1H and Supplementary Figure S2). In summary, SYHA1813 exhibited robust antitumor activities across a panel of genetically and histologically heterogeneous KRAS-mutated tumor models, including the model resistant to AMG510.
We then asked whether SYHA1813 could suppress the growth of tumors carrying EGFR mutations or resistant to EGFR tyrosine kinase inhibitors (TKIs). To address this question, we initially employed the NCI-H1975 model containing EGFRL858R/T790M mutation, which is resistant to the first-generation EGFR TKIs, and found that SYHA1813 significantly suppressed the tumor growth (Figure 1I). Then, we evaluated the activity of SYHA1813 against the tumor model carrying EGFRC797S triple mutation (PC-9-OR) that is resistant to third-generation EGFR TKIs [7]. As shown in Figure 1J, osimertinib (AZD9291), the first FDA approved third-generation EGFR TKI, failed to inhibit tumor growth even at the dose of 10 mg/kg. However, we observed a significant deceleration with SYHA1813 in tumor growth rate at doses of 5 and 10 mg/kg (Figure 1J). Furthermore, we employed the osimertinib-resistant tumor (designated as AZDR) [8] and also observed significant suppression upon SYHA1813 monotherapy (Figure 1K). Similarly, in another resistant model (designated as 67R) to the third-generation EGFR TKI ASK120067 [8], SYHA1813 monotherapy inhibited tumor growth (Figure 1L). The IHC results also demonstrated a reduction in angiogenic and macrophage markers in tumor tissues following SYHA1813 administration (Supplementary Figure S3). These findings demonstrated that SYHA1813 exhibited potent antitumor activity in different EGFR TKI-resistant models.
Given that the response rates to immunotherapy are quite limited across most tumor types, including those carrying KRAS mutations, and importantly, angiogenesis and macrophages have been identified as key factors involved in the resistance to immunotherapy [9], we then validated whether SYHA1813 could enhance the antitumor activity of anti-PD-1 therapy in immunocompetent mice models bearing CT26 (KRASG12D mutation) and MC38 (KRASWT) colon cancer (Figure 1M-N). In both models, monotherapy with anti-PD-1 antibody or SYHA1813 yielded moderate to marked suppression of tumor growth, while the combination of SYHA1813 and anti-PD-1 antibody conferred significant advantages over each monotherapy group. In the CT26 and MC38 models, the combinational ratio was 1.88 and 1.42, respectively, both exceeding 1, indicative of a synergistic effect (Supplementary Table S1). Flow cytometry analysis revealed that the combination therapy significantly reduced F4/80+ and CD206+ macrophages (Figure 1O). Additionally, a noticeable increase of CD8+ T cells was observed in the combination treatment group, along with an upregulation of granzyme B expression (Figure 1P), indicating an enhanced cytotoxic response against tumor cells.
Our study discovered the activities of SYHA1813 in KRAS- or EGFR-mutated tumors, providing support for further investigation of SYHA1813. Given potential variations in the response of subcutaneous tumors and other tumor types to angiogenic agents, further experiments in orthotopic models will be conducted. The findings in the current work highlight the feasibility of a therapeutic strategy targeting the tumor microenvironment, which can be applied to treat oncogene-driven cancers and overcome the challenge of drug resistance to targeted therapy.
Hua Xie, Jian Ding, Wenhu Duan, and Meiyu Geng supervised the project. Yingqiang Liu, Linjiang Tong, Mengge Zhang, Mengzhen Lai, Fang Feng, Haotian Tang, Yi Chen, and Yan Li conducted the experiments. Yingqiang Liu, Mengge Zhang, Qi Zhang and Qiupei Liu analyzed the data. Yingqiang Liu, Qiupei Liu, Hua Xie, Jian Ding, and Wenhu Duan wrote the manuscript.
The authors declare no potential conflicts of interest.
This research was supported by grants from the Natural Science Foundation of China for Innovation Research Group (81821005), the National Natural Science Foundation of China (82273948, 81573271 and 81903638), High-level Innovative Research Institute (2021B0909050003), State Key Laboratory of Drug Research (SKLDR-2023-TT-01 and SIMM2205KF-09), Lingang Laboratory (LG202103-02-02), and Institutes for Drug Discovery and Development, Chinese Academy of Sciences (CASIMM0120225003-1 and -2).
Animal experiments containing cell line-derived xenografts and patient-derived xenografts were carried out in accordance with the Guide for the Care and Use of Laboratory Animals and approved by the Institutional Animal Care and Use Committee of Shanghai Institute of Materia Medica (approval number 2021-04-DJ-59).
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


