Safety and Effectiveness of Antidysrhythmic Drugs for Pharmacologic Cardioversion of Recent-Onset Atrial Fibrillation: a Systematic Review and Bayesian Network Meta-analysis.
Ian S deSouza, Pragati Shrestha, Robert Allen, Jessica Koos, Henry Thode
{"title":"Safety and Effectiveness of Antidysrhythmic Drugs for Pharmacologic Cardioversion of Recent-Onset Atrial Fibrillation: a Systematic Review and Bayesian Network Meta-analysis.","authors":"Ian S deSouza, Pragati Shrestha, Robert Allen, Jessica Koos, Henry Thode","doi":"10.1007/s10557-024-07552-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The available evidence to determine which antidysrhythmic drug is superior for pharmacologic cardioversion of recent-onset (onset within 48 h) atrial fibrillation (AF) is uncertain. We aimed to identify the safest and most effective agent for pharmacologic cardioversion of recent-onset AF in the emergency department.</p><p><strong>Methods: </strong>We searched MEDLINE, Embase, and Web of Science from inception to February 21, 2023 (PROSPERO: CRD42018083781). Eligible studies were randomized controlled trials that enrolled adult participants with AF ≤ 48 h, compared a guideline-recommended antidysrhythmic drug with another antidysrhythmic drug or a different formulation of the same drug or placebo and reported specific adverse events. The primary outcome was immediate, serious adverse event - cardiac arrest, sustained ventricular tachydysrhythmia, atrial flutter 1:1 atrioventricular conduction, hypotension, and bradycardia. Additional analyses included the outcomes of conversion to sinus rhythm within 4 h and 24 h. We extracted data according to PRISMA-NMA and appraised trials using Cochrane RoB 2. We performed Bayesian network meta-analysis (NMA) using a Markov Chain Monte Carlo method with random-effect model and vague prior distribution to calculate odds ratios with 95% credible intervals. We assessed confidence using CINeMA. We used surface under the cumulative ranking curve (SUCRA) to rank agent(s).</p><p><strong>Results: </strong>The systematic review initially identified 5545 studies. Twenty-five studies met eligibility criteria, and 22 studies (n = 3082) provided data for NMA, which demonstrated that vernakalant (SUCRA = 70.9%) is most likely to be safest. Additional effectiveness NMA demonstrated that flecainide (SUCRA = 89.0%) is most likely to be superior for conversion within 4 h (27 studies; n = 2681), and ranolazine-amiodarone IV (SUCRA 93.7%) is most likely to be superior for conversion within 24 h (24 studies; n = 3213). Confidence in the NMA estimates is variable and limited mostly by within-study bias and imprecision.</p><p><strong>Conclusions: </strong>Among guideline-recommended antidysrhythmic drugs, the combination of digoxin IV and amiodarone IV is definitely among the least safe for cardioversion of recent onset AF; flecainide, vernakalant, ibutilide, propafenone, and amiodarone IV are definitely among the most effective for cardioversion within 4 h; flecainide is definitely among the most effective for cardioversion within 24 h. Further, randomized controlled trials with predetermined and strictly defined, hemodynamic adverse event outcomes are recommended.</p>","PeriodicalId":9557,"journal":{"name":"Cardiovascular Drugs and Therapy","volume":" ","pages":"903-923"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Drugs and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10557-024-07552-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The available evidence to determine which antidysrhythmic drug is superior for pharmacologic cardioversion of recent-onset (onset within 48 h) atrial fibrillation (AF) is uncertain. We aimed to identify the safest and most effective agent for pharmacologic cardioversion of recent-onset AF in the emergency department.
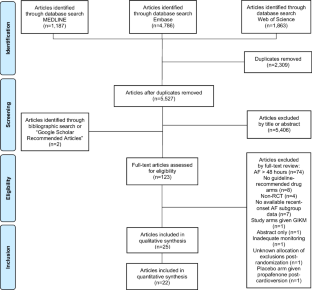
Methods: We searched MEDLINE, Embase, and Web of Science from inception to February 21, 2023 (PROSPERO: CRD42018083781). Eligible studies were randomized controlled trials that enrolled adult participants with AF ≤ 48 h, compared a guideline-recommended antidysrhythmic drug with another antidysrhythmic drug or a different formulation of the same drug or placebo and reported specific adverse events. The primary outcome was immediate, serious adverse event - cardiac arrest, sustained ventricular tachydysrhythmia, atrial flutter 1:1 atrioventricular conduction, hypotension, and bradycardia. Additional analyses included the outcomes of conversion to sinus rhythm within 4 h and 24 h. We extracted data according to PRISMA-NMA and appraised trials using Cochrane RoB 2. We performed Bayesian network meta-analysis (NMA) using a Markov Chain Monte Carlo method with random-effect model and vague prior distribution to calculate odds ratios with 95% credible intervals. We assessed confidence using CINeMA. We used surface under the cumulative ranking curve (SUCRA) to rank agent(s).
Results: The systematic review initially identified 5545 studies. Twenty-five studies met eligibility criteria, and 22 studies (n = 3082) provided data for NMA, which demonstrated that vernakalant (SUCRA = 70.9%) is most likely to be safest. Additional effectiveness NMA demonstrated that flecainide (SUCRA = 89.0%) is most likely to be superior for conversion within 4 h (27 studies; n = 2681), and ranolazine-amiodarone IV (SUCRA 93.7%) is most likely to be superior for conversion within 24 h (24 studies; n = 3213). Confidence in the NMA estimates is variable and limited mostly by within-study bias and imprecision.
Conclusions: Among guideline-recommended antidysrhythmic drugs, the combination of digoxin IV and amiodarone IV is definitely among the least safe for cardioversion of recent onset AF; flecainide, vernakalant, ibutilide, propafenone, and amiodarone IV are definitely among the most effective for cardioversion within 4 h; flecainide is definitely among the most effective for cardioversion within 24 h. Further, randomized controlled trials with predetermined and strictly defined, hemodynamic adverse event outcomes are recommended.
期刊介绍:
Designed to objectively cover the process of bench to bedside development of cardiovascular drug, device and cell therapy, and to bring you the information you need most in a timely and useful format, Cardiovascular Drugs and Therapy takes a fresh and energetic look at advances in this dynamic field.
Homing in on the most exciting work being done on new therapeutic agents, Cardiovascular Drugs and Therapy focusses on developments in atherosclerosis, hyperlipidemia, diabetes, ischemic syndromes and arrhythmias. The Journal is an authoritative source of current and relevant information that is indispensable for basic and clinical investigators aiming for novel, breakthrough research as well as for cardiologists seeking to best serve their patients.
Providing you with a single, concise reference tool acknowledged to be among the finest in the world, Cardiovascular Drugs and Therapy is listed in Web of Science and PubMed/Medline among other abstracting and indexing services. The regular articles and frequent special topical issues equip you with an up-to-date source defined by the need for accurate information on an ever-evolving field. Cardiovascular Drugs and Therapy is a careful and accurate guide through the maze of new products and therapies which furnishes you with the details on cardiovascular pharmacology that you will refer to time and time again.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


