{"title":"The impact of platelet-to-lymphocyte ratio on clinical outcomes in heart failure: a systematic review and meta-analysis.","authors":"Mehrbod Vakhshoori, Niloofar Bondariyan, Sadeq Sabouhi, Keivan Kiani, Nazanin Alaei Faradonbeh, Sayed Ali Emami, Mehrnaz Shakarami, Farbod Khanizadeh, Shahin Sanaei, Niloofaralsadat Motamedi, Davood Shafie","doi":"10.1177/17539447241227287","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Inflammation has been suggested to play a role in heart failure (HF) pathogenesis. However, the role of platelet-to-lymphocyte ratio (PLR), as a novel biomarker, to assess HF prognosis needs to be investigated. We sought to evaluate the impact of PLR on HF clinical outcomes.</p><p><strong>Methods: </strong>English-published records in PubMed/Medline, Scopus, and Web-of-science databases were screened until December 2023. Relevant articles evaluated PLR with clinical outcomes (including mortality, rehospitalization, HF worsening, and HF detection) were recruited, with PLR difference analysis based on death/survival status in total and HF with reduced ejection fraction (HFrEF) patients.</p><p><strong>Results: </strong>In total, 21 articles (<i>n</i> = 13,924) were selected. The total mean age was 70.36 ± 12.88 years (males: 61.72%). Mean PLR was 165.54 [95% confidence interval (CI): 154.69-176.38]. In total, 18 articles (<i>n</i> = 10,084) reported mortality [either follow-up (PLR: 162.55, 95% CI: 149.35-175.75) or in-hospital (PLR: 192.83, 95% CI: 150.06-235.61) death rate] and the mean PLR was 166.68 (95% CI: 154.87-178.50). Further analysis revealed PLR was significantly lower in survived HF patients rather than deceased group (152.34, 95% CI: 134.01-170.68 <i>versus</i> 194.73, 95% CI: 175.60-213.85, standard mean difference: -0.592, 95% CI: -0.857 to -0.326, <i>p</i> < 0.001). A similar trend was observed for HFrEF patients. PLR failed to show any association with mortality risk (hazard ratio: 1.02, 95% CI: 0.99-1.05, <i>p</i> = 0.289). Analysis of other aforementioned outcomes was not possible due to the presence of few studies of interest.</p><p><strong>Conclusion: </strong>PLR should be used with caution for prognosis assessment in HF sufferers and other studies are necessary to explore the exact association.</p>","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"18 ","pages":"17539447241227287"},"PeriodicalIF":2.2000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10838041/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17539447241227287","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Inflammation has been suggested to play a role in heart failure (HF) pathogenesis. However, the role of platelet-to-lymphocyte ratio (PLR), as a novel biomarker, to assess HF prognosis needs to be investigated. We sought to evaluate the impact of PLR on HF clinical outcomes.
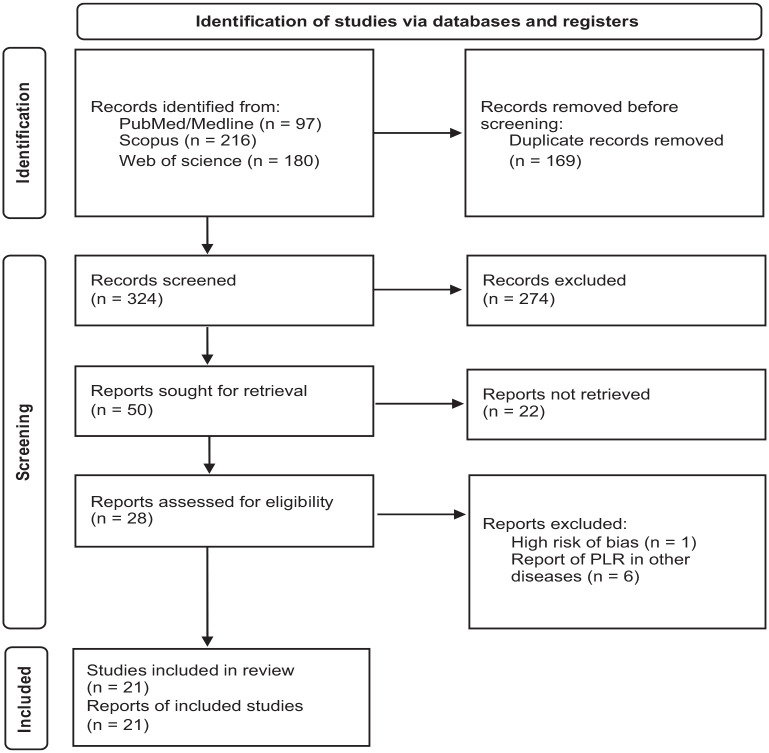
Methods: English-published records in PubMed/Medline, Scopus, and Web-of-science databases were screened until December 2023. Relevant articles evaluated PLR with clinical outcomes (including mortality, rehospitalization, HF worsening, and HF detection) were recruited, with PLR difference analysis based on death/survival status in total and HF with reduced ejection fraction (HFrEF) patients.
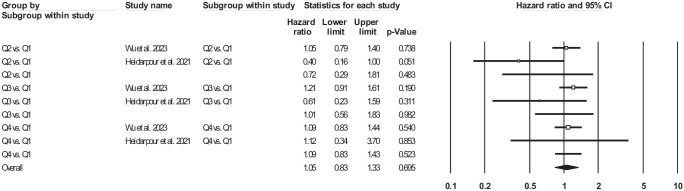
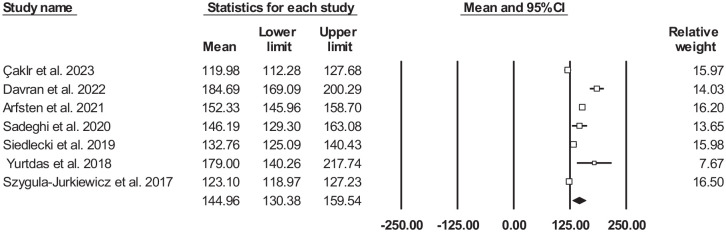
Results: In total, 21 articles (n = 13,924) were selected. The total mean age was 70.36 ± 12.88 years (males: 61.72%). Mean PLR was 165.54 [95% confidence interval (CI): 154.69-176.38]. In total, 18 articles (n = 10,084) reported mortality [either follow-up (PLR: 162.55, 95% CI: 149.35-175.75) or in-hospital (PLR: 192.83, 95% CI: 150.06-235.61) death rate] and the mean PLR was 166.68 (95% CI: 154.87-178.50). Further analysis revealed PLR was significantly lower in survived HF patients rather than deceased group (152.34, 95% CI: 134.01-170.68 versus 194.73, 95% CI: 175.60-213.85, standard mean difference: -0.592, 95% CI: -0.857 to -0.326, p < 0.001). A similar trend was observed for HFrEF patients. PLR failed to show any association with mortality risk (hazard ratio: 1.02, 95% CI: 0.99-1.05, p = 0.289). Analysis of other aforementioned outcomes was not possible due to the presence of few studies of interest.
Conclusion: PLR should be used with caution for prognosis assessment in HF sufferers and other studies are necessary to explore the exact association.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


