Sarah Jänsch, Dimitar Evdokimov, Nadine Egenolf, Caren Meyer Zu Altenschildesche, Luisa Kreß, Nurcan Üçeyler
{"title":"Distinguishing fibromyalgia syndrome from small fiber neuropathy: a clinical guide.","authors":"Sarah Jänsch, Dimitar Evdokimov, Nadine Egenolf, Caren Meyer Zu Altenschildesche, Luisa Kreß, Nurcan Üçeyler","doi":"10.1097/PR9.0000000000001136","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Fibromyalgia syndrome (FMS) and small fiber neuropathy (SFN) are distinct pain conditions that share commonalities and may be challenging as for differential diagnosis.</p><p><strong>Objective: </strong>To comprehensively investigate clinical characteristics of women with FMS and SFN to determine clinically applicable parameters for differentiation.</p><p><strong>Methods: </strong>We retrospectively analyzed medical records of 158 women with FMS and 53 with SFN focusing on pain-specific medical and family history, accompanying symptoms, additional diseases, and treatment. We investigated data obtained using standardized pain, depression, and anxiety questionnaires. We further analyzed test results and findings obtained in standardized small fiber tests.</p><p><strong>Results: </strong>FMS patients were on average ten years younger at symptom onset, described higher pain intensities requiring frequent change of pharmaceutics, and reported generalized pain compared to SFN. Pain in FMS was accompanied by irritable bowel or sleep disturbances, and in SFN by paresthesias, numbness, and impaired glucose metabolism (<i>P</i> < 0.01 each). Family history was informative for chronic pain and affective disorders in FMS (<i>P</i> < 0.001) and for neurological disorders in SFN patients (<i>P</i> < 0.001). Small fiber pathology in terms of skin denervation and/or thermal sensory threshold elevation was present in 110/158 (69.7 %) FMS patients and 39/53 (73.6 %) SFN patients. FMS patients mainly showed proximally reduced skin innervation and higher corneal nerve branch densities (p<0.001) whereas SFN patients were characterized by reduced cold detection and prolonged electrical A-delta conduction latencies (<i>P</i> < 0.05).</p><p><strong>Conclusions: </strong>Our data show that FMS and SFN differ substantially. Detailed pain, drug and family history, investigating blood glucose metabolism, and applying differential small fiber tests may help to improve diagnostic differentiation and targeted therapy.</p>","PeriodicalId":52189,"journal":{"name":"Pain Reports","volume":"9 1","pages":"e1136"},"PeriodicalIF":3.1000,"publicationDate":"2024-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10811691/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pain Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/PR9.0000000000001136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Fibromyalgia syndrome (FMS) and small fiber neuropathy (SFN) are distinct pain conditions that share commonalities and may be challenging as for differential diagnosis.
Objective: To comprehensively investigate clinical characteristics of women with FMS and SFN to determine clinically applicable parameters for differentiation.
Methods: We retrospectively analyzed medical records of 158 women with FMS and 53 with SFN focusing on pain-specific medical and family history, accompanying symptoms, additional diseases, and treatment. We investigated data obtained using standardized pain, depression, and anxiety questionnaires. We further analyzed test results and findings obtained in standardized small fiber tests.
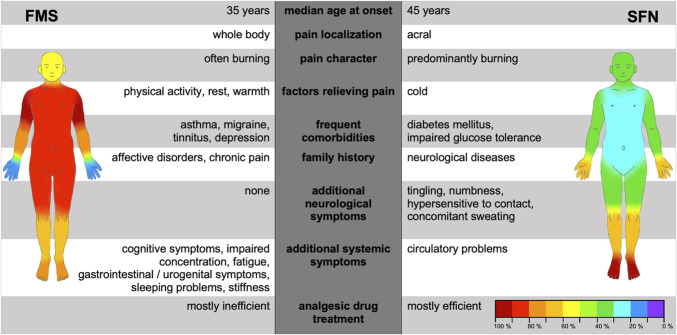
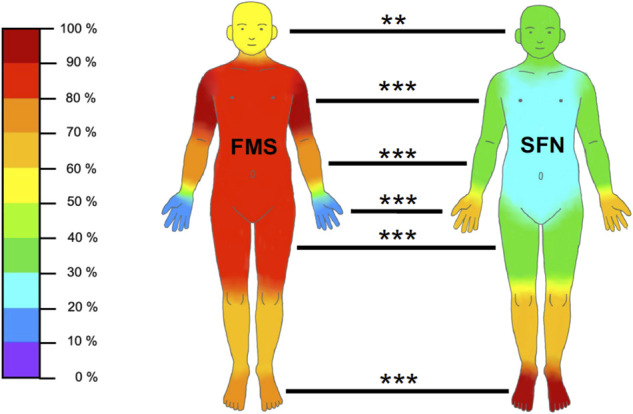
Results: FMS patients were on average ten years younger at symptom onset, described higher pain intensities requiring frequent change of pharmaceutics, and reported generalized pain compared to SFN. Pain in FMS was accompanied by irritable bowel or sleep disturbances, and in SFN by paresthesias, numbness, and impaired glucose metabolism (P < 0.01 each). Family history was informative for chronic pain and affective disorders in FMS (P < 0.001) and for neurological disorders in SFN patients (P < 0.001). Small fiber pathology in terms of skin denervation and/or thermal sensory threshold elevation was present in 110/158 (69.7 %) FMS patients and 39/53 (73.6 %) SFN patients. FMS patients mainly showed proximally reduced skin innervation and higher corneal nerve branch densities (p<0.001) whereas SFN patients were characterized by reduced cold detection and prolonged electrical A-delta conduction latencies (P < 0.05).
Conclusions: Our data show that FMS and SFN differ substantially. Detailed pain, drug and family history, investigating blood glucose metabolism, and applying differential small fiber tests may help to improve diagnostic differentiation and targeted therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


