Xiaoyu Ren, Haoran Li, Kaihang Xu, Zhongkai Li, Bin Gao, Wangsheng Lu, Guangming Yang, Yunjie Wang, Yin Yin, Tao Chen
{"title":"Hemodynamic study on the therapeutic effects of varying diameter embolic coils in the treatment of intracranial aneurysms","authors":"Xiaoyu Ren, Haoran Li, Kaihang Xu, Zhongkai Li, Bin Gao, Wangsheng Lu, Guangming Yang, Yunjie Wang, Yin Yin, Tao Chen","doi":"10.1002/cnm.3807","DOIUrl":null,"url":null,"abstract":"<p>Endovascular coiling is the predominant method for treating cerebral aneurysms. Extensive reports on selecting coil length, hardness, and material are available. However, the impact of coil diameter on postoperative outcomes remains unclear. This study enrolled six personalized geometric models of intracranial aneurysms: three bifurcation aneurysms and three sidewall aneurysms. Four coil models were constructed by changing the coil diameter. Coil embolization was simulated using the finite element method. Computational fluid dynamics was used to characterize hemodynamics in the aneurysms after embolization. Evaluation parameters included velocity reduction, wall shear stress (WSS), low WSS (LWSS), oscillatory shear index (OSI), relative residence time (RRT), and residual flow volume in the aneurysms. At the peak time (<i>t</i> = 0.17 s), the proportion of LWSS area in bifurcation aneurysms increase with the rise in coil diameter: 0.8D, 71.28 ± 12.62% versus 1D, 74.97 ± 19.17% versus 1.2D, 78.88 ± 18.56% versus 1.4D, 84.00 ± 11.53% (mean ± SD). The proportion of high OSI area decreases as the coil diameter increases: 0.8D, 4.41% ± 2.82% versus 1.0D, 3.78 ± 3.33% versus 1.2D, 2.28% ± 1.77% versus 1.4D, 1.58% ± 1.11% (mean ± SD). The proportion of high RRT area increases as the coil diameter rises: 0.8D, 3.40% ± 1.68% versus 1.0D, 7.67 ± 4.12% versus 1.2D, 9.84% ± 9.50% versus 1.4D, 22.29% ± 14.28% (mean ± SD). Side wall aneurysms do not exhibit the aforementioned trend. Bifurcation aneurysms plugged with a coil of 1.4 times the diameter have the largest RFVs (<10 mm/s) within the group. Aforementioned patterns are not found in sidewall aneurysms. In the treatment of aneurysms with coiling, varying coil diameters can result in different hemodynamic environments within the aneurysm. Larger coil diameters have improved hemodynamic performance for bifurcation aneurysms. However, coil diameter and embolization effectiveness have no significant relationship for sidewall aneurysms.</p>","PeriodicalId":50349,"journal":{"name":"International Journal for Numerical Methods in Biomedical Engineering","volume":"40 3","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2024-01-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal for Numerical Methods in Biomedical Engineering","FirstCategoryId":"5","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cnm.3807","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
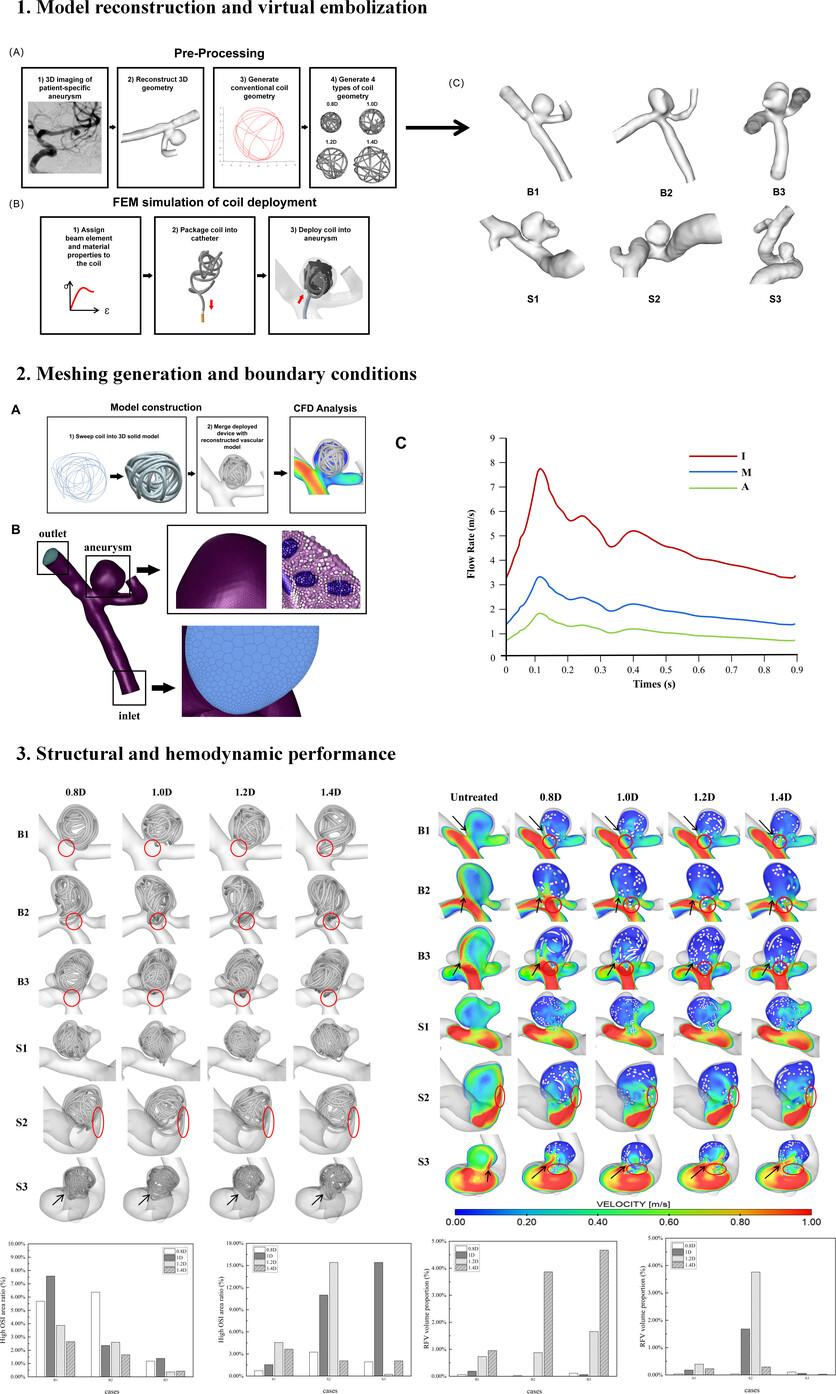
Endovascular coiling is the predominant method for treating cerebral aneurysms. Extensive reports on selecting coil length, hardness, and material are available. However, the impact of coil diameter on postoperative outcomes remains unclear. This study enrolled six personalized geometric models of intracranial aneurysms: three bifurcation aneurysms and three sidewall aneurysms. Four coil models were constructed by changing the coil diameter. Coil embolization was simulated using the finite element method. Computational fluid dynamics was used to characterize hemodynamics in the aneurysms after embolization. Evaluation parameters included velocity reduction, wall shear stress (WSS), low WSS (LWSS), oscillatory shear index (OSI), relative residence time (RRT), and residual flow volume in the aneurysms. At the peak time (t = 0.17 s), the proportion of LWSS area in bifurcation aneurysms increase with the rise in coil diameter: 0.8D, 71.28 ± 12.62% versus 1D, 74.97 ± 19.17% versus 1.2D, 78.88 ± 18.56% versus 1.4D, 84.00 ± 11.53% (mean ± SD). The proportion of high OSI area decreases as the coil diameter increases: 0.8D, 4.41% ± 2.82% versus 1.0D, 3.78 ± 3.33% versus 1.2D, 2.28% ± 1.77% versus 1.4D, 1.58% ± 1.11% (mean ± SD). The proportion of high RRT area increases as the coil diameter rises: 0.8D, 3.40% ± 1.68% versus 1.0D, 7.67 ± 4.12% versus 1.2D, 9.84% ± 9.50% versus 1.4D, 22.29% ± 14.28% (mean ± SD). Side wall aneurysms do not exhibit the aforementioned trend. Bifurcation aneurysms plugged with a coil of 1.4 times the diameter have the largest RFVs (<10 mm/s) within the group. Aforementioned patterns are not found in sidewall aneurysms. In the treatment of aneurysms with coiling, varying coil diameters can result in different hemodynamic environments within the aneurysm. Larger coil diameters have improved hemodynamic performance for bifurcation aneurysms. However, coil diameter and embolization effectiveness have no significant relationship for sidewall aneurysms.
期刊介绍:
All differential equation based models for biomedical applications and their novel solutions (using either established numerical methods such as finite difference, finite element and finite volume methods or new numerical methods) are within the scope of this journal. Manuscripts with experimental and analytical themes are also welcome if a component of the paper deals with numerical methods. Special cases that may not involve differential equations such as image processing, meshing and artificial intelligence are within the scope. Any research that is broadly linked to the wellbeing of the human body, either directly or indirectly, is also within the scope of this journal.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


