{"title":"Metabolic acidosis in chronic kidney disease: mere consequence or also culprit?","authors":"Christian Kuhn, Nilufar Mohebbi, Alexander Ritter","doi":"10.1007/s00424-024-02912-5","DOIUrl":null,"url":null,"abstract":"<p><p>Metabolic acidosis is a frequent complication in non-transplant chronic kidney disease (CKD) and after kidney transplantation. It occurs when net endogenous acid production exceeds net acid excretion. While nephron loss with reduced ammoniagenesis is the main cause of acid retention in non-transplant CKD patients, additional pathophysiological mechanisms are likely inflicted in kidney transplant recipients. Functional tubular damage by calcineurin inhibitors seems to play a key role causing renal tubular acidosis. Notably, experimental and clinical studies over the past decades have provided evidence that metabolic acidosis may not only be a consequence of CKD but also a driver of disease. In metabolic acidosis, activation of hormonal systems and the complement system resulting in fibrosis have been described. Further studies of changes in renal metabolism will likely contribute to a deeper understanding of the pathophysiology of metabolic acidosis in CKD. While alkali supplementation in case of reduced serum bicarbonate < 22 mmol/l has been endorsed by CKD guidelines for many years to slow renal functional decline, among other considerations, beneficial effects and thresholds for treatment have lately been under intense debate. This review article discusses this topic in light of the most recent results of trials assessing the efficacy of dietary and pharmacological interventions in CKD and kidney transplant patients.</p>","PeriodicalId":19954,"journal":{"name":"Pflugers Archiv : European journal of physiology","volume":null,"pages":null},"PeriodicalIF":2.9000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11006741/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pflugers Archiv : European journal of physiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00424-024-02912-5","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHYSIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
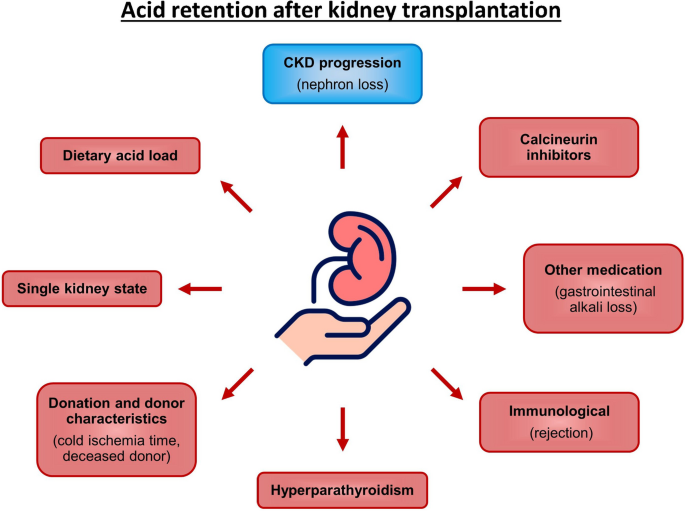
Metabolic acidosis is a frequent complication in non-transplant chronic kidney disease (CKD) and after kidney transplantation. It occurs when net endogenous acid production exceeds net acid excretion. While nephron loss with reduced ammoniagenesis is the main cause of acid retention in non-transplant CKD patients, additional pathophysiological mechanisms are likely inflicted in kidney transplant recipients. Functional tubular damage by calcineurin inhibitors seems to play a key role causing renal tubular acidosis. Notably, experimental and clinical studies over the past decades have provided evidence that metabolic acidosis may not only be a consequence of CKD but also a driver of disease. In metabolic acidosis, activation of hormonal systems and the complement system resulting in fibrosis have been described. Further studies of changes in renal metabolism will likely contribute to a deeper understanding of the pathophysiology of metabolic acidosis in CKD. While alkali supplementation in case of reduced serum bicarbonate < 22 mmol/l has been endorsed by CKD guidelines for many years to slow renal functional decline, among other considerations, beneficial effects and thresholds for treatment have lately been under intense debate. This review article discusses this topic in light of the most recent results of trials assessing the efficacy of dietary and pharmacological interventions in CKD and kidney transplant patients.
期刊介绍:
Pflügers Archiv European Journal of Physiology publishes those results of original research that are seen as advancing the physiological sciences, especially those providing mechanistic insights into physiological functions at the molecular and cellular level, and clearly conveying a physiological message. Submissions are encouraged that deal with the evaluation of molecular and cellular mechanisms of disease, ideally resulting in translational research. Purely descriptive papers covering applied physiology or clinical papers will be excluded. Papers on methodological topics will be considered if they contribute to the development of novel tools for further investigation of (patho)physiological mechanisms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


