Clinical outcomes and end-of-life treatment in 596 patients with isolated traumatic brain injury: a retrospective comparison of two Dutch level-I trauma centers.
Menco J S Niemeyer, Denise Jochems, Jan C Van Ditshuizen, Janneke de Kanter, Lotte Cremers, Martijn van Hattem, Dennis Den Hartog, Roderick Marijn Houwert, Luke P H Leenen, Karlijn J P van Wessem
{"title":"Clinical outcomes and end-of-life treatment in 596 patients with isolated traumatic brain injury: a retrospective comparison of two Dutch level-I trauma centers.","authors":"Menco J S Niemeyer, Denise Jochems, Jan C Van Ditshuizen, Janneke de Kanter, Lotte Cremers, Martijn van Hattem, Dennis Den Hartog, Roderick Marijn Houwert, Luke P H Leenen, Karlijn J P van Wessem","doi":"10.1007/s00068-023-02407-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>With an increasingly older population and rise in incidence of traumatic brain injury (TBI), end-of-life decisions have become frequent. This study investigated the rate of withdrawal of life sustaining treatment (WLST) and compared treatment outcomes in patients with isolated TBI in two Dutch level-I trauma centers.</p><p><strong>Methods: </strong>From 2011 to 2016, a retrospective cohort study of patients aged ≥ 18 years with isolated moderate-to-severe TBI (Abbreviated Injury Scale (AIS) head ≥ 3) was conducted at the University Medical Center Rotterdam (UMC-R) and the University Medical Center Utrecht (UMC-U). Demographics, radiologic injury characteristics, clinical outcomes, and functional outcomes at 3-6 months post-discharge were collected.</p><p><strong>Results: </strong>The study population included 596 patients (UMC-R: n = 326; UMC-U: n = 270). There were no statistical differences in age, gender, mechanism of injury, and radiologic parameters between both institutes. UMC-R patients had a higher AIShead (UMC-R: 5 [4-5] vs. UMC-U: 4 [4-5], p < 0.001). There was no difference in the prehospital Glasgow Coma Scale (GCS). However, UMC-R patients had lower GCSs in the Emergency Department and used more prehospital sedation. Total in-hospital mortality was 29% (n = 170), of which 71% (n = 123) occurred after WLST. Two percent (n = 10) remained in unresponsive wakefulness syndrome (UWS) state during follow-up.</p><p><strong>Discussion: </strong>This study demonstrated a high WLST rate among deceased patients with isolated TBI. Demographics and outcomes were similar for both centers even though AIShead was significantly higher in UMC-R patients. Possibly, prehospital sedation might have influenced AIS coding. Few patients persisted in UWS. Further research is needed on WLST patients in a broader spectrum of ethics, culture, and complex medical profiles, as it is a growing practice in modern critical care.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>","PeriodicalId":12064,"journal":{"name":"European Journal of Trauma and Emergency Surgery","volume":" ","pages":"1249-1259"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11458745/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Trauma and Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00068-023-02407-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/16 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: With an increasingly older population and rise in incidence of traumatic brain injury (TBI), end-of-life decisions have become frequent. This study investigated the rate of withdrawal of life sustaining treatment (WLST) and compared treatment outcomes in patients with isolated TBI in two Dutch level-I trauma centers.
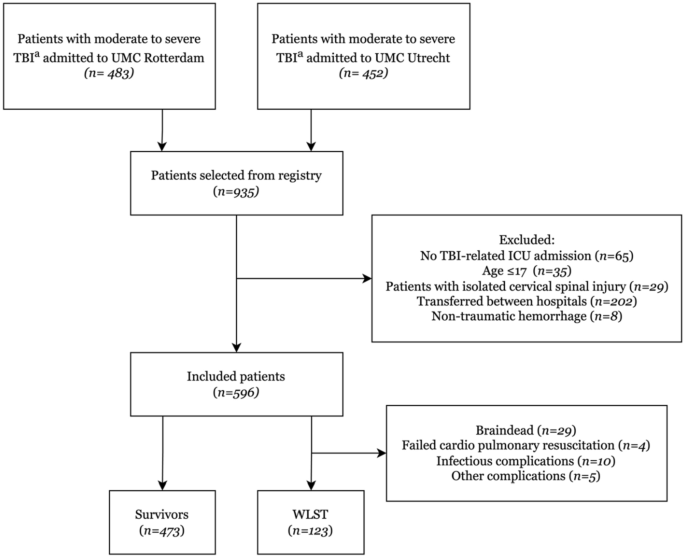
Methods: From 2011 to 2016, a retrospective cohort study of patients aged ≥ 18 years with isolated moderate-to-severe TBI (Abbreviated Injury Scale (AIS) head ≥ 3) was conducted at the University Medical Center Rotterdam (UMC-R) and the University Medical Center Utrecht (UMC-U). Demographics, radiologic injury characteristics, clinical outcomes, and functional outcomes at 3-6 months post-discharge were collected.
Results: The study population included 596 patients (UMC-R: n = 326; UMC-U: n = 270). There were no statistical differences in age, gender, mechanism of injury, and radiologic parameters between both institutes. UMC-R patients had a higher AIShead (UMC-R: 5 [4-5] vs. UMC-U: 4 [4-5], p < 0.001). There was no difference in the prehospital Glasgow Coma Scale (GCS). However, UMC-R patients had lower GCSs in the Emergency Department and used more prehospital sedation. Total in-hospital mortality was 29% (n = 170), of which 71% (n = 123) occurred after WLST. Two percent (n = 10) remained in unresponsive wakefulness syndrome (UWS) state during follow-up.
Discussion: This study demonstrated a high WLST rate among deceased patients with isolated TBI. Demographics and outcomes were similar for both centers even though AIShead was significantly higher in UMC-R patients. Possibly, prehospital sedation might have influenced AIS coding. Few patients persisted in UWS. Further research is needed on WLST patients in a broader spectrum of ethics, culture, and complex medical profiles, as it is a growing practice in modern critical care.
Level of evidence: Level III, retrospective cohort study.
期刊介绍:
The European Journal of Trauma and Emergency Surgery aims to open an interdisciplinary forum that allows for the scientific exchange between basic and clinical science related to pathophysiology, diagnostics and treatment of traumatized patients. The journal covers all aspects of clinical management, operative treatment and related research of traumatic injuries.
Clinical and experimental papers on issues relevant for the improvement of trauma care are published. Reviews, original articles, short communications and letters allow the appropriate presentation of major and minor topics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


