Roux-en-Y Gastric Bypass Versus One Anastomosis Gastric Bypass as Revisional Surgery After Failed Sleeve Gastrectomy: A Systematic Review and Meta-analysis.
Karim Ataya, Al Moutuz Al Jaafreh, Hussein El Bourji, Ayman Bsat, Hussein Nassar, Amir Al Ayoubi, George Abi Saad
{"title":"Roux-en-Y Gastric Bypass Versus One Anastomosis Gastric Bypass as Revisional Surgery After Failed Sleeve Gastrectomy: A Systematic Review and Meta-analysis.","authors":"Karim Ataya, Al Moutuz Al Jaafreh, Hussein El Bourji, Ayman Bsat, Hussein Nassar, Amir Al Ayoubi, George Abi Saad","doi":"10.17476/jmbs.2023.12.2.57","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to assess the outcomes of revisional procedures, namely Roux-en-Y gastric bypass (RYGB) and one anastomosis gastric bypass (OAGB) following unsuccessful laparoscopic sleeve gastrectomy.</p><p><strong>Materials and methods: </strong>This systematic review and meta-analysis included 817 patients (404 in OAGB group, 413 in RYGB group) from seven retrospective comparative studies. Data on sample size, demographics, perioperative complications, operative time, pre- and post-revisional body mass index, total weight loss, and global weight loss over follow-up were extracted.</p><p><strong>Results: </strong>The mean operative time was 98.2-201 minutes for RYGB versus 78.7-168 minutes for OAGB. Despite classical RYGB gastric bypass taking longer, mini gastric bypass resulted in greater weight loss than RYGB, with a mean difference of -5.84 (95% confidence interval [CI], -6.74 to -4.94; P<0.00001; I<sup>2</sup>=0%), greater total weight loss, and a higher diabetes remission rate (odds ratio [OR], 0.32; 95% CI, 0.14 to 0.71). However, OAGB was associated with a significantly higher incidence of postoperative gastroesophageal reflux than RYGB (52 vs. 31: OR, 0.40; 95% CI, 0.24 to 0.67; P=0.0005; I<sup>2</sup>=0%).</p><p><strong>Conclusion: </strong>OAGB was performed more quickly and boasted greater total weight loss and higher diabetes remission rates compared to RYGB after failed sleeve gastrectomy. However, OAGB also demonstrated a higher incidence of postoperative gastroesophageal reflux disease. Thus, careful patient selection is essential when considering OAGB.</p><p><strong>Trial registration: </strong>PROSPERO Identifier: CRD42023474966.</p>","PeriodicalId":73828,"journal":{"name":"Journal of metabolic and bariatric surgery","volume":"12 2","pages":"57-66"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10771971/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of metabolic and bariatric surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17476/jmbs.2023.12.2.57","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/29 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aimed to assess the outcomes of revisional procedures, namely Roux-en-Y gastric bypass (RYGB) and one anastomosis gastric bypass (OAGB) following unsuccessful laparoscopic sleeve gastrectomy.
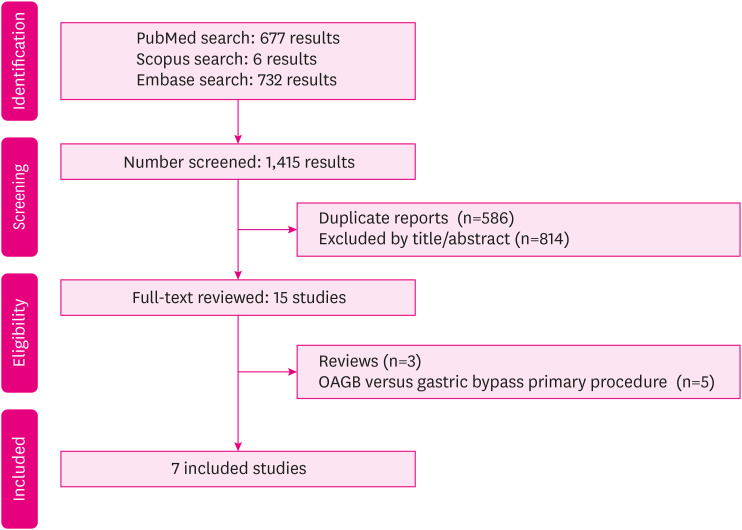
Materials and methods: This systematic review and meta-analysis included 817 patients (404 in OAGB group, 413 in RYGB group) from seven retrospective comparative studies. Data on sample size, demographics, perioperative complications, operative time, pre- and post-revisional body mass index, total weight loss, and global weight loss over follow-up were extracted.
Results: The mean operative time was 98.2-201 minutes for RYGB versus 78.7-168 minutes for OAGB. Despite classical RYGB gastric bypass taking longer, mini gastric bypass resulted in greater weight loss than RYGB, with a mean difference of -5.84 (95% confidence interval [CI], -6.74 to -4.94; P<0.00001; I2=0%), greater total weight loss, and a higher diabetes remission rate (odds ratio [OR], 0.32; 95% CI, 0.14 to 0.71). However, OAGB was associated with a significantly higher incidence of postoperative gastroesophageal reflux than RYGB (52 vs. 31: OR, 0.40; 95% CI, 0.24 to 0.67; P=0.0005; I2=0%).
Conclusion: OAGB was performed more quickly and boasted greater total weight loss and higher diabetes remission rates compared to RYGB after failed sleeve gastrectomy. However, OAGB also demonstrated a higher incidence of postoperative gastroesophageal reflux disease. Thus, careful patient selection is essential when considering OAGB.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


