Risk indicators for gingival recession in the esthetic zone: A cross-sectional clinical, tomographic, and ultrasonographic study
Abstract
Background
To evaluate the risk indicators associated with midfacial gingival recessions (GR) in the natural dentition esthetic regions.
Methods
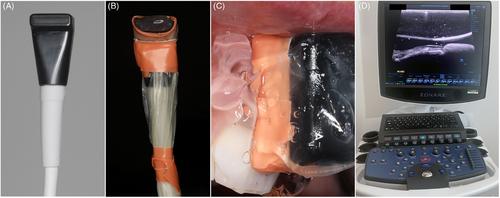
Cone-beam computed tomography (CBCT) results of thirty-seven subjects presenting with 268 eligible teeth were included in the cross-sectional study. Clinical measurements included presence/absence of midfacial GR; the depth of the midfacial, mesial, and distal gingival recession; the recession type (RT); keratinized tissue width (KT); and attached gingiva width (AG). Questionnaires were utilized to capture patient-reported esthetics and dental hypersensitivity for each study tooth. Buccal bone dehiscence (cBBD) and buccal bone thickness (cBBT) were measured on the CBCT scans. High-frequency ultrasonography was performed to assess gingival thickness (GT) and buccal bone dehiscence (uBBD). Intraoral optical scanning was obtained to quantify the buccolingual position of each study site (3D profile analysis). Multilevel logistic regression analyses with generalized estimation equations were performed to assess the factors associated with the conditions of interest.
Results
The presence of midfacial GR was significantly associated with the history of periodontal treatment for pocket reduction (OR 7.99, p = 0.006), KT (OR 0.62, p < 0.001), cBBD (OR 2.30, p = 0.015), GT 1.5 mm from the gingival margin (OR 0.18, p = 0.04) and 3D profile 1 mm from the gingival margin (OR 1.04, p = 0.001). The depth of midfacial GR was significantly correlated to previous history of periodontal treatment (OR 0.96, p = 0.001), KT (OR −0.18, p < 0.001), presence of bone fenestration (OR 0.24, p = 0.044), and cBBD (OR 0.43, p < 0.001). The depth of midfacial GR was also the only factor associated with patient-reported esthetics (OR −3.38, p = 0.022), while KT (OR 0.77, p = 0.018) and AG (OR 0.82, p = 0.047) were significantly correlated with patient-reported dental hypersensitivity.
Conclusions
Several risk indicators of midfacial and interproximal GR in the esthetic region were identified. The use of imaging technologies allowed for detection of parameters associated with the conditions of interest, and, therefore, their incorporation in future clinical studies is advocated. Ultrasonography could be preferred over CBCT for a noninvasive assessment of periodontal phenotype.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


