{"title":"Prognostic Value of Neutrophils-to-Lymphocytes Ratio and Platelets-to-Lymphocytes Ratio in Sepsis Patients With Lymphopenia.","authors":"Xianming Qiu, Quanzhen Wang, Yuke Zhang, Qiannan Zhao, Zhiming Jiang, Lei Zhou","doi":"10.1177/11772719231223156","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Inflammation plays a critical role in sepsis. The integration of neutrophil-to-lymphocyte ratio (NLR) and platelets-to-lymphocytes ratio (PLR) from multiple cell types offers a novel approach to rapidly assess inflammation status. However, the predictive role of NLR and PLR in sepsis with lymphopenia remains uncertain.</p><p><strong>Objectives: </strong>The purpose of this study was to explore the prognostic value of NLR and PLR in sepsis patients with lymphopenia.</p><p><strong>Design and methods: </strong>In this observational retrospective study, we included 172 sepsis patients with lymphopenia and collected clinical characteristics for analysis. Through binary logistic regression analysis, we identified independent factors. Receiver-operating characteristic curves (ROC) and areas under the curves (AUC) were employed to assess the ability to predict hospital mortality risk.</p><p><strong>Results: </strong>Our results showed a total hospital mortality rate of 53.49%. Multivariate analysis demonstrated that NLR (OR = 1.11, <i>P</i> < .001) and PLR (OR = 1.01, <i>P</i> = .003) were independent predictors associated with hospital mortality in sepsis patients with lymphopenia. The AUCs of NLR and PLR were 0.750 (95% CI: 0.634-0.788, <i>P</i> < .001) and 0.662 (95% CI: 0.580-0.743, <i>P</i> < .001), respectively. Notably, an optimal cut-off value of 18.93 for NLR displayed a sensitivity of 75.0% and specificity of 63.0% in discriminating hospital mortality in sepsis patients with lymphopenia, while the optimal cut-off value for PLR was 377.50, with a sensitivity of 67.5% and specificity of 64.1%.</p><p><strong>Conclusion: </strong>NLR and PLR serve as independent predictors of hospital mortality in sepsis patients with lymphopenia.</p>","PeriodicalId":47060,"journal":{"name":"Biomarker Insights","volume":"19 ","pages":"11772719231223156"},"PeriodicalIF":2.6000,"publicationDate":"2024-01-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10768602/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomarker Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11772719231223156","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Inflammation plays a critical role in sepsis. The integration of neutrophil-to-lymphocyte ratio (NLR) and platelets-to-lymphocytes ratio (PLR) from multiple cell types offers a novel approach to rapidly assess inflammation status. However, the predictive role of NLR and PLR in sepsis with lymphopenia remains uncertain.
Objectives: The purpose of this study was to explore the prognostic value of NLR and PLR in sepsis patients with lymphopenia.
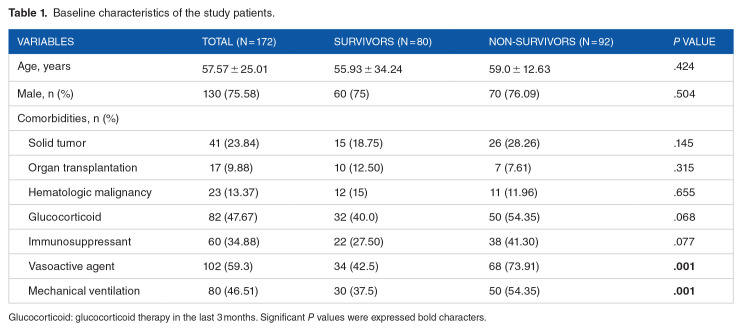
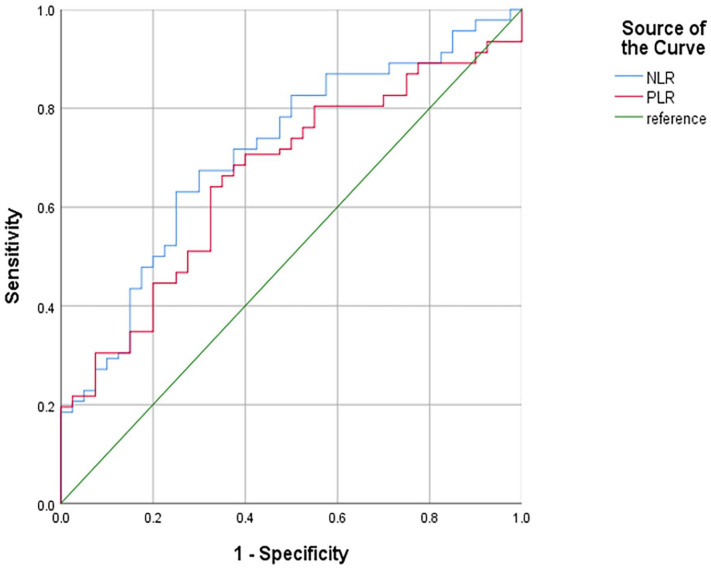
Design and methods: In this observational retrospective study, we included 172 sepsis patients with lymphopenia and collected clinical characteristics for analysis. Through binary logistic regression analysis, we identified independent factors. Receiver-operating characteristic curves (ROC) and areas under the curves (AUC) were employed to assess the ability to predict hospital mortality risk.
Results: Our results showed a total hospital mortality rate of 53.49%. Multivariate analysis demonstrated that NLR (OR = 1.11, P < .001) and PLR (OR = 1.01, P = .003) were independent predictors associated with hospital mortality in sepsis patients with lymphopenia. The AUCs of NLR and PLR were 0.750 (95% CI: 0.634-0.788, P < .001) and 0.662 (95% CI: 0.580-0.743, P < .001), respectively. Notably, an optimal cut-off value of 18.93 for NLR displayed a sensitivity of 75.0% and specificity of 63.0% in discriminating hospital mortality in sepsis patients with lymphopenia, while the optimal cut-off value for PLR was 377.50, with a sensitivity of 67.5% and specificity of 64.1%.
Conclusion: NLR and PLR serve as independent predictors of hospital mortality in sepsis patients with lymphopenia.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


