{"title":"Key nodal stations for predicting splenic hilar nodal metastasis in upper advanced gastric cancer without invasion of the greater curvature","authors":"Masashi Nishino, Takaki Yoshikawa, Masahiro Yura, Rei Ogawa, Ryota Sakon, Kenichi Ishizu, Takeyuki Wada, Tsutomu Hayashi, Yukinori Yamagata","doi":"10.1002/ags3.12759","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Standard surgery for upper advanced gastric cancer without invasion of the greater curvature (UGC-GC) is spleen-preserving D2 total gastrectomy without dissection of the splenic-hilar nodes (#10). However, some patients with nodal metastasis to #10 survive more than 5 years due to nodal dissection of #10. If nodal metastasis to #10 is predictable based on the positivity of other nodes dissected by the current standard surgery without #10 nodal dissection, physicians may be able to consider #10 dissection.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This study retrospectively reviewed data from the National Cancer Center Hospital in Japan between 2000 and 2012. We selected cases that met the following criteria: (1) D2 or more total gastrectomy with splenectomy, (2) UGC-GC, and (3) histological type is gastric adenocarcinoma. We performed univariate and multivariate analyses concerning lymph node stations associated with #10 metastasis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 366 patients were examined. A multivariate analysis revealed that #10 metastasis was associated with positivity of the nodes along the short gastric arteries (#4sa) and distal nodes along the splenic artery (#11d) (#4sa: <i>p</i> = 0.003, #11d: <i>p</i> = 0.016). When either key node was positive, the metastatic rate of #10 was 24.4%, and the therapeutic value index was 13.3.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>#4sa and #11d were key lymph nodes predicting #10 nodal metastasis in UGC-GC. When these key nodes are positive on computed tomography before surgery or according to a rapid pathological examination during surgery, dissection of #10 should be considered even if upper advanced tumors are not invading the greater curvature.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 3","pages":"413-419"},"PeriodicalIF":3.3000,"publicationDate":"2023-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12759","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12759","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Standard surgery for upper advanced gastric cancer without invasion of the greater curvature (UGC-GC) is spleen-preserving D2 total gastrectomy without dissection of the splenic-hilar nodes (#10). However, some patients with nodal metastasis to #10 survive more than 5 years due to nodal dissection of #10. If nodal metastasis to #10 is predictable based on the positivity of other nodes dissected by the current standard surgery without #10 nodal dissection, physicians may be able to consider #10 dissection.
Methods
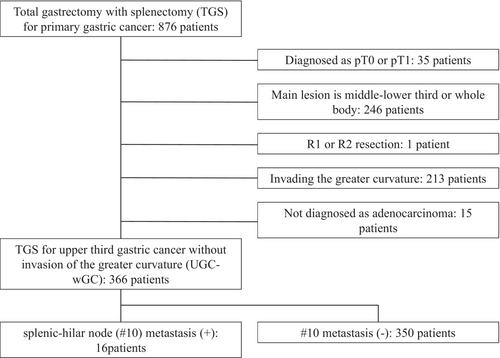
This study retrospectively reviewed data from the National Cancer Center Hospital in Japan between 2000 and 2012. We selected cases that met the following criteria: (1) D2 or more total gastrectomy with splenectomy, (2) UGC-GC, and (3) histological type is gastric adenocarcinoma. We performed univariate and multivariate analyses concerning lymph node stations associated with #10 metastasis.
Results
A total of 366 patients were examined. A multivariate analysis revealed that #10 metastasis was associated with positivity of the nodes along the short gastric arteries (#4sa) and distal nodes along the splenic artery (#11d) (#4sa: p = 0.003, #11d: p = 0.016). When either key node was positive, the metastatic rate of #10 was 24.4%, and the therapeutic value index was 13.3.
Conclusions
#4sa and #11d were key lymph nodes predicting #10 nodal metastasis in UGC-GC. When these key nodes are positive on computed tomography before surgery or according to a rapid pathological examination during surgery, dissection of #10 should be considered even if upper advanced tumors are not invading the greater curvature.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


