Alexander M. Tucker, Peter J. Madsen, Shih-Shan Lang, Phillip B. Storm
{"title":"Technical note: Traumatic atlanto-occipital dislocation and severe subaxial cervical distraction injury in an infant","authors":"Alexander M. Tucker, Peter J. Madsen, Shih-Shan Lang, Phillip B. Storm","doi":"10.1038/s41394-023-00612-3","DOIUrl":null,"url":null,"abstract":"<h3 data-test=\"abstract-sub-heading\">Introduction</h3><p>Traumatic injuries of the spine requiring surgery are rare in infancy. Fusion procedures in the very young are not well-described at the atlanto-occipital junction or subaxial spine. Here we describe novel segmental posterior instrumentation in a severe spinal column disruption in an infant.</p><h3 data-test=\"abstract-sub-heading\">Case presentation</h3><p>A 13-month-old male with atlanto-occipital dislocation and severe C6-7 distraction (ASIA impairment scale A) presented after a motor vehicle accident. He underwent instrumented fusion (occiput-C2 and C6-7) and halo placement. Postoperative imaging demonstrated reduction of the C6-7 vertebral bodies. Physical examination showed lower limb paraplegia and preserved upper extremity strength except for mild weakness in hand grip (3/5 on the MRC grading scale). Occiput-C2 instrumentation was performed using occipital keel and C2 pedicle screws with sublaminar C1 polyester tape. C6-7 reduction and fixation was performed with laminar hooks. Arthrodesis was promoted with lineage-committed cellular bone matrix allograft and suboccipital autograft. Anterior column stabilization was deferred secondary to a CSF leak. Intraoperative monitoring was performed throughout the procedure. Within 1 month after surgery the patient was able to manipulate objects against gravity. CT imaging revealed bony fusion and spontaneous reduction of C6-7.</p><h3 data-test=\"abstract-sub-heading\">Discussion</h3><p>Spinal instrumentation is technically challenging in infants, regardless of injury mechanism, particularly in cases with complete spinal column disruption, but an anterior fusion may be avoided in infants and small children with posterior stabilization and halo placement.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"2 1","pages":""},"PeriodicalIF":0.9000,"publicationDate":"2024-01-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-023-00612-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Traumatic injuries of the spine requiring surgery are rare in infancy. Fusion procedures in the very young are not well-described at the atlanto-occipital junction or subaxial spine. Here we describe novel segmental posterior instrumentation in a severe spinal column disruption in an infant.
Case presentation
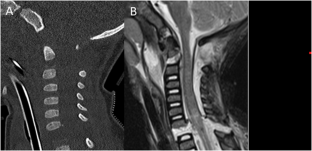
A 13-month-old male with atlanto-occipital dislocation and severe C6-7 distraction (ASIA impairment scale A) presented after a motor vehicle accident. He underwent instrumented fusion (occiput-C2 and C6-7) and halo placement. Postoperative imaging demonstrated reduction of the C6-7 vertebral bodies. Physical examination showed lower limb paraplegia and preserved upper extremity strength except for mild weakness in hand grip (3/5 on the MRC grading scale). Occiput-C2 instrumentation was performed using occipital keel and C2 pedicle screws with sublaminar C1 polyester tape. C6-7 reduction and fixation was performed with laminar hooks. Arthrodesis was promoted with lineage-committed cellular bone matrix allograft and suboccipital autograft. Anterior column stabilization was deferred secondary to a CSF leak. Intraoperative monitoring was performed throughout the procedure. Within 1 month after surgery the patient was able to manipulate objects against gravity. CT imaging revealed bony fusion and spontaneous reduction of C6-7.
Discussion
Spinal instrumentation is technically challenging in infants, regardless of injury mechanism, particularly in cases with complete spinal column disruption, but an anterior fusion may be avoided in infants and small children with posterior stabilization and halo placement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


