Adam Diamond, Sunil Karhadkar, Kenneth Chavin, Serban Constantinescu, Kwan N Lau, Oscar Perez-Leal, Kerry Mohrien, Nicole Sifontis, Antonio Di Carlo
{"title":"Dosing strategies for <i>de novo</i> once-daily extended release tacrolimus in kidney transplant recipients based on <i>CYP3A5</i> genotype.","authors":"Adam Diamond, Sunil Karhadkar, Kenneth Chavin, Serban Constantinescu, Kwan N Lau, Oscar Perez-Leal, Kerry Mohrien, Nicole Sifontis, Antonio Di Carlo","doi":"10.5500/wjt.v13.i6.368","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tacrolimus extended-release tablets have been Food and Drug Administration-approved for use in the <i>de novo</i> kidney transplant population. Dosing requi rements often vary for tacrolimus based on several factors including variation in metabolism based on <i>CYP3A5</i> expression. Patients who express <i>CYP3A5</i> often require higher dosing of immediate-release tacrolimus, but this has not been established for tacrolimus extended-release tablets in the <i>de novo</i> setting.</p><p><strong>Aim: </strong>To obtain target trough concentrations of extended-release tacrolimus in <i>de novo</i> kidney transplant recipients according to <i>CYP3A5</i> genotype.</p><p><strong>Methods: </strong>Single-arm, prospective, single-center, open-label, observational study (ClinicalTrials.gov: NCT037 13645). Life cycle pharma tacrolimus (LCPT) orally once daily at a starting dose of 0.13 mg/kg/day based on actual body weight. If weight is more than 120% of ideal body weight, an adjusted body weight was used. LCPT dose was adjusted to maintain tacrolimus trough concentrations of 8-10 ng/mL. Pharmacogenetic analysis of <i>CYP3A5</i> genotype was performed at study conclusion.</p><p><strong>Results: </strong>Mean time to therapeutic tacrolimus trough concentration was longer in <i>CYP3A5</i> intermediate and extensive metabolizers <i>vs CYP3A5</i> non-expressers (6 d <i>vs</i> 13.5 d <i>vs</i> 4.5 d; <i>P</i> = 0.025). Mean tacrolimus doses and weight-based doses to achieve therapeutic concentration were higher in <i>CYP3A5</i> intermediate and extensive metabolizers <i>vs CYP3A5</i> non-expressers (16 mg <i>vs</i> 16 mg <i>vs</i> 12 mg; <i>P</i> = 0.010) (0.20 mg/kg <i>vs</i> 0.19 mg/kg <i>vs</i> 0.13 mg/kg; <i>P</i> = 0.018). <i>CYP3A5</i> extensive metabolizers experienced lower mean tacrolimus trough concentrations throughout the study period compared to <i>CYP3A5</i> intermediate metabolizers and non-expressers (7.98 ng/mL <i>vs</i> 9.18 ng/mL <i>vs</i> 10.78 ng/mL; <i>P</i> = 0 0.008). No differences were identified with regards to kidney graft function at 30-d post-transplant. Serious adverse events were reported for 13 (36%) patients.</p><p><strong>Conclusion: </strong>Expression of <i>CYP3A5</i> leads to higher starting doses and incremental dosage titration of extended-release tacro limus to achieve target trough concentrations. We suggest a higher starting dose of 0.2 mg/kg/d for <i>CYP3A5</i> expressers.</p>","PeriodicalId":65557,"journal":{"name":"世界移植杂志","volume":"13 6","pages":"368-378"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10758687/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5500/wjt.v13.i6.368","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Tacrolimus extended-release tablets have been Food and Drug Administration-approved for use in the de novo kidney transplant population. Dosing requi rements often vary for tacrolimus based on several factors including variation in metabolism based on CYP3A5 expression. Patients who express CYP3A5 often require higher dosing of immediate-release tacrolimus, but this has not been established for tacrolimus extended-release tablets in the de novo setting.
Aim: To obtain target trough concentrations of extended-release tacrolimus in de novo kidney transplant recipients according to CYP3A5 genotype.
Methods: Single-arm, prospective, single-center, open-label, observational study (ClinicalTrials.gov: NCT037 13645). Life cycle pharma tacrolimus (LCPT) orally once daily at a starting dose of 0.13 mg/kg/day based on actual body weight. If weight is more than 120% of ideal body weight, an adjusted body weight was used. LCPT dose was adjusted to maintain tacrolimus trough concentrations of 8-10 ng/mL. Pharmacogenetic analysis of CYP3A5 genotype was performed at study conclusion.
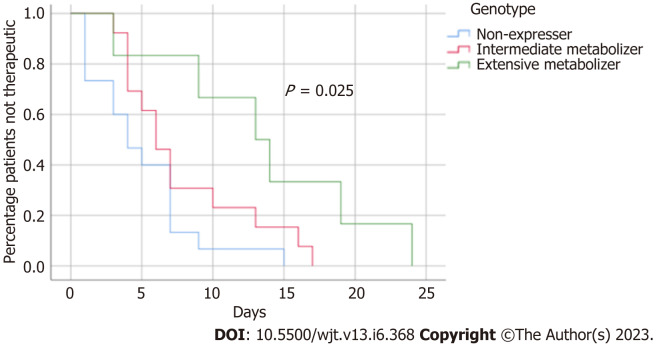
Results: Mean time to therapeutic tacrolimus trough concentration was longer in CYP3A5 intermediate and extensive metabolizers vs CYP3A5 non-expressers (6 d vs 13.5 d vs 4.5 d; P = 0.025). Mean tacrolimus doses and weight-based doses to achieve therapeutic concentration were higher in CYP3A5 intermediate and extensive metabolizers vs CYP3A5 non-expressers (16 mg vs 16 mg vs 12 mg; P = 0.010) (0.20 mg/kg vs 0.19 mg/kg vs 0.13 mg/kg; P = 0.018). CYP3A5 extensive metabolizers experienced lower mean tacrolimus trough concentrations throughout the study period compared to CYP3A5 intermediate metabolizers and non-expressers (7.98 ng/mL vs 9.18 ng/mL vs 10.78 ng/mL; P = 0 0.008). No differences were identified with regards to kidney graft function at 30-d post-transplant. Serious adverse events were reported for 13 (36%) patients.
Conclusion: Expression of CYP3A5 leads to higher starting doses and incremental dosage titration of extended-release tacro limus to achieve target trough concentrations. We suggest a higher starting dose of 0.2 mg/kg/d for CYP3A5 expressers.
背景:他克莫司缓释片已获美国食品和药物管理局批准用于新肾移植患者。他克莫司的剂量要求往往因多种因素而异,包括因 CYP3A5 表达而异的代谢。表达 CYP3A5 的患者通常需要更高的速释他克莫司剂量,但在新肾移植患者中,他克莫司缓释片的剂量要求尚未确定。目的:根据 CYP3A5 基因型,获得新肾移植受者中他克莫司缓释片的目标谷浓度:单臂、前瞻性、单中心、开放标签、观察性研究(ClinicalTrials.gov:NCT037 13645)。生命周期制药公司他克莫司(LCPT)口服,每天一次,起始剂量为 0.13 毫克/千克/天,以实际体重为基础。如果体重超过理想体重的 120%,则使用调整后的体重。调整 LCPT 剂量以维持他克莫司谷浓度在 8-10 纳克/毫升。研究结束时进行了 CYP3A5 基因型的药物遗传学分析:结果:CYP3A5中间代谢者和广泛代谢者与CYP3A5非表达者相比,达到治疗性他克莫司谷浓度的平均时间更长(6 d vs 13.5 d vs 4.5 d; P = 0.025)。CYP3A5中间代谢者和广泛代谢者与CYP3A5非表达者相比,达到治疗浓度的平均他克莫司剂量和基于体重的剂量更高(16毫克 vs 16毫克 vs 12毫克;P = 0.010)(0.20毫克/千克 vs 0.19毫克/千克 vs 0.13毫克/千克;P = 0.018)。在整个研究期间,CYP3A5广泛代谢者的他克莫司平均谷浓度低于CYP3A5中等代谢者和非表达者(7.98纳克/毫升 vs 9.18纳克/毫升 vs 10.78纳克/毫升;P = 0.008)。移植后 30 天的肾移植功能无差异。13例(36%)患者出现严重不良事件:结论:CYP3A5的表达导致缓释他克莫司的起始剂量较高,并需要递增剂量滴定以达到目标谷浓度。我们建议 CYP3A5 表达者的起始剂量为 0.2 mg/kg/d。
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


