{"title":"Motor band sign or biomarker","authors":"Sadegh Ghaderi, Sana Mohammadi","doi":"10.1002/ird3.43","DOIUrl":null,"url":null,"abstract":"<p>Motor neuron diseases (MNDs), such as amyotrophic lateral sclerosis (ALS), are a group of devastating and progressive neurodegenerative disorders that affect the upper and lower motor neurons (UMN and LMN) [<span>1</span>]. Other forms of MND include primary lateral sclerosis (PLS), progressive muscular atrophy, progressive bulbar palsy, spinal muscular atrophy, and frontotemporal dementia-MND [<span>2</span>]. Early and accurate diagnosis is critical; yet the diagnosis and prognosis of MNDs are challenging due to the complexity and heterogeneity of these diseases. Therefore, there is a need for sensitive, suggestive, and reliable biomarkers to detect and monitor the progression of neurodegeneration and neuroinflammation in MNDs [<span>1</span>].</p><p>The motor band sign (MBS), described as a curvilinear “band” of hypointensity in the precentral gyrus (and primary motor cortex [M1 area]) in susceptibility-weighted images generated from gradient-echo pulse sequences (GRE/SWI) or the GRE-T2*-weighted image, is considered a magnetic resonance imaging (MRI) biomarker of UMN involvement in MNDs, such as ALS and PLS (Figure 1) [<span>1, 3</span>]. The sensitivity of SWI is particularly high when it comes to detecting deoxygenated blood and mineral deposits within the brain [<span>4</span>]. The MBS has also been observed in other neurodegenerative movement disorders [<span>1, 5, 6</span>], such as Parkinson's disease [<span>5-7</span>], Alzhimer's disease [<span>5-8</span>], and Huntington's disease [<span>9</span>].</p><p>The exact cause of MBS is not yet fully comprehended, but it is widely believed to result from an accumulation of iron in the motor cortex due to the degeneration of microglia [<span>1</span>]. The suspected basis is increased cortical iron deposition and microglial activity in UMN regions as supported by neuroimaging and neuropathological studies [<span>10</span>].</p><p>Mohammadi and Ghaderi (2023) provide a comprehensive review of the literature for the growing body of evidence supporting the utility of MRI for detecting characteristic changes in MNDs with a focus on the MBS [<span>1</span>]. The study found that the presence of MBS, observed as a hypointensity area along the precentral gyri, is linked to the severity of UMN impairment in patients with MNDs. The study highlighted a strong association between MBS and the severity of UMN impairment [<span>1</span>]. This builds on previous work demonstrating the specificity of MBS for ALS and PLS compared to healthy controls [<span>3</span>].</p><p>Quantitative MRI techniques like quantitative susceptibility mapping (QSM) allow sensitive quantification of iron deposition and have shown promise for accurately detecting MBS in MNDs [<span>1</span>]. Compared to conventional MRI techniques, such as T2-weighted (T2-w), T2*-w, and R2* relaxation, susceptibility imaging including QSM and SWI offers superior sensitivity to iron accumulation in the motor cortex [<span>4</span>]. As mentioned in previous studies, the extent of cortical hypointensities on SWI correlates with disease severity and progression over time in ALS patients [<span>3, 4</span>].</p><p>Together, these findings strongly support the use of SWI and QSM for detecting cortical metrics and biomarkers of UMN degeneration in MNDs in both research and clinical settings. Given the lack of reliable diagnostic and prognostic MRI biomarkers in these diseases, optimizing MRI protocols to include SWI and/or QSM sequences could provide valuable insights into disease pathophysiology and progression. As suggested by Mohammadi and Ghaderi [<span>1</span>], the presence of MBS on SWI/QSM should prompt close monitoring for emerging MND.</p><p>MR neuroimaging biomarkers and prognostic indicators such as MBS in SWI/QSM that closely reflect disease progression can serve as outcome measures in clinical trials [<span>1</span>]. These collective findings strongly advocate for the inclusion of SWI and QSM in routine clinical MRI protocols. The detection of characteristic cortical changes in advanced MRI techniques, particularly MBS on SWI/QSM, shows great promise as an objective marker of UMN impairment severity and progression. These quantitative MRI biomarkers have the potential to significantly impact prognosis, diagnosis, and treatment trials in this critically underserved patient population. The concept of MBS as a hallmark of ALS is gaining clinical acceptance, and the adoption of SWI/QSM into routine protocols is recommended to capitalize on these advanced imaging insights.</p><p>For maximum clinical utility, further clinical research with larger prospective cohorts is needed to determine the sensitivity, specificity, and predictive values of MBS for diagnosis across various subtypes of MND and different stages of the disease. Longitudinal and prospective multicenter studies that track changes over time and correlation with clinical metrics will help establish prognostic values. In addition, multimodal MRI combining structural, functional, metabolic, and quantitative techniques may offer the best imaging biomarkers though the optimization of feasible protocols for clinical use is needed.</p><p>Sadegh Ghaderi and Sana Mohammadi analyzed the data and prepared the first draft of the manuscript. Sadegh Ghaderi participated in the conception and design of the study; Sadegh Ghaderi and Sana Mohammadi constructively revised the manuscript; Sana Mohammadi participated in data collection and organization; Sadegh Ghaderi participated in and supervised the study throughout, and they share corresponding authorship. All authors commented on previous versions of the manuscript and approved the final version.</p><p>The authors declare no conflict of interest.</p><p>Not applicable.</p><p>Not applicable.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"1 4","pages":"378-380"},"PeriodicalIF":0.0000,"publicationDate":"2023-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.43","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.43","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Motor neuron diseases (MNDs), such as amyotrophic lateral sclerosis (ALS), are a group of devastating and progressive neurodegenerative disorders that affect the upper and lower motor neurons (UMN and LMN) [1]. Other forms of MND include primary lateral sclerosis (PLS), progressive muscular atrophy, progressive bulbar palsy, spinal muscular atrophy, and frontotemporal dementia-MND [2]. Early and accurate diagnosis is critical; yet the diagnosis and prognosis of MNDs are challenging due to the complexity and heterogeneity of these diseases. Therefore, there is a need for sensitive, suggestive, and reliable biomarkers to detect and monitor the progression of neurodegeneration and neuroinflammation in MNDs [1].
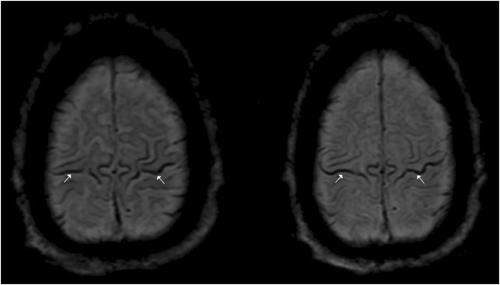
The motor band sign (MBS), described as a curvilinear “band” of hypointensity in the precentral gyrus (and primary motor cortex [M1 area]) in susceptibility-weighted images generated from gradient-echo pulse sequences (GRE/SWI) or the GRE-T2*-weighted image, is considered a magnetic resonance imaging (MRI) biomarker of UMN involvement in MNDs, such as ALS and PLS (Figure 1) [1, 3]. The sensitivity of SWI is particularly high when it comes to detecting deoxygenated blood and mineral deposits within the brain [4]. The MBS has also been observed in other neurodegenerative movement disorders [1, 5, 6], such as Parkinson's disease [5-7], Alzhimer's disease [5-8], and Huntington's disease [9].
The exact cause of MBS is not yet fully comprehended, but it is widely believed to result from an accumulation of iron in the motor cortex due to the degeneration of microglia [1]. The suspected basis is increased cortical iron deposition and microglial activity in UMN regions as supported by neuroimaging and neuropathological studies [10].
Mohammadi and Ghaderi (2023) provide a comprehensive review of the literature for the growing body of evidence supporting the utility of MRI for detecting characteristic changes in MNDs with a focus on the MBS [1]. The study found that the presence of MBS, observed as a hypointensity area along the precentral gyri, is linked to the severity of UMN impairment in patients with MNDs. The study highlighted a strong association between MBS and the severity of UMN impairment [1]. This builds on previous work demonstrating the specificity of MBS for ALS and PLS compared to healthy controls [3].
Quantitative MRI techniques like quantitative susceptibility mapping (QSM) allow sensitive quantification of iron deposition and have shown promise for accurately detecting MBS in MNDs [1]. Compared to conventional MRI techniques, such as T2-weighted (T2-w), T2*-w, and R2* relaxation, susceptibility imaging including QSM and SWI offers superior sensitivity to iron accumulation in the motor cortex [4]. As mentioned in previous studies, the extent of cortical hypointensities on SWI correlates with disease severity and progression over time in ALS patients [3, 4].
Together, these findings strongly support the use of SWI and QSM for detecting cortical metrics and biomarkers of UMN degeneration in MNDs in both research and clinical settings. Given the lack of reliable diagnostic and prognostic MRI biomarkers in these diseases, optimizing MRI protocols to include SWI and/or QSM sequences could provide valuable insights into disease pathophysiology and progression. As suggested by Mohammadi and Ghaderi [1], the presence of MBS on SWI/QSM should prompt close monitoring for emerging MND.
MR neuroimaging biomarkers and prognostic indicators such as MBS in SWI/QSM that closely reflect disease progression can serve as outcome measures in clinical trials [1]. These collective findings strongly advocate for the inclusion of SWI and QSM in routine clinical MRI protocols. The detection of characteristic cortical changes in advanced MRI techniques, particularly MBS on SWI/QSM, shows great promise as an objective marker of UMN impairment severity and progression. These quantitative MRI biomarkers have the potential to significantly impact prognosis, diagnosis, and treatment trials in this critically underserved patient population. The concept of MBS as a hallmark of ALS is gaining clinical acceptance, and the adoption of SWI/QSM into routine protocols is recommended to capitalize on these advanced imaging insights.
For maximum clinical utility, further clinical research with larger prospective cohorts is needed to determine the sensitivity, specificity, and predictive values of MBS for diagnosis across various subtypes of MND and different stages of the disease. Longitudinal and prospective multicenter studies that track changes over time and correlation with clinical metrics will help establish prognostic values. In addition, multimodal MRI combining structural, functional, metabolic, and quantitative techniques may offer the best imaging biomarkers though the optimization of feasible protocols for clinical use is needed.
Sadegh Ghaderi and Sana Mohammadi analyzed the data and prepared the first draft of the manuscript. Sadegh Ghaderi participated in the conception and design of the study; Sadegh Ghaderi and Sana Mohammadi constructively revised the manuscript; Sana Mohammadi participated in data collection and organization; Sadegh Ghaderi participated in and supervised the study throughout, and they share corresponding authorship. All authors commented on previous versions of the manuscript and approved the final version.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


