Single-stage versus two-stage bone flap reconstruction in chronic osteomyelitis: Multicenter outcomes comparison
Abstract
Background
Chronic osteomyelitis is an invalidating disease, and its severity grows according to the infection's particular features. The Cierny-Maiden criteria classify it according to the anatomical aspects (I to IV) and also by physiological class (A host being in good immune condition and B hosts being locally (L) or systemically (S) compromised). The surgical approach to chronic osteomyelitis involves radical debridement and dead space reconstruction. Two-stage management with delayed reconstruction is the most common surgical management, while one-stage treatment with concomitant reconstruction is a more aggressive approach with less available literature. Which method gives the best results is unclear. The purpose of this study is to compare single and two-stage techniques.
Methods
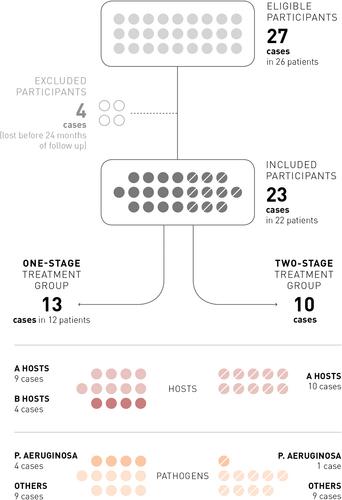
The authors carried out a retrospective multicentric cohort study to compare two primary outcomes (bone union and infection healing) in one versus two-stage reconstructions with vascularized bone flaps in 23 cases of limb osteomyelitis (22 patients, 23 extremities). Thirteen subjects (56.5%) sustained a single-stage treatment consisting of a single surgery of radical debridement, concomitant soft tissue coverage, and bone reconstruction. Ten cases (43.5%) sustained a two-stage approach: radical debridement, simultaneous primary soft tissue closure, and antibiotic PMMA spacers implanted in 7 patients.
Results
No statistical differences were observed between one- and two-stage approaches in bone union rate and infection recurrence risk. Even though bone union seems to be higher and faster in the two-stage than in the one-stage group, and all infection relapses occurred in the one-stage group, data did not statistically confirm these differences. Two of the six cases (33.3%) of bone nonunion occurred in compromised hosts (representing only 17.4% of our sample). The B-hosts bone union rate was 50.0%, while it reached 78.9% in A-hosts, but the difference was not statistically significant (p = .5392). Infection recurrence was higher in B-hosts than in A-hosts (p = .0086) and in Pseudomonas aeruginosa sustained infections (p = .0208), but in the latter case, the treatment strategy did not influence the outcome (p = .4000).
Conclusions
Bone union and infection healing rates are comparable between one and two-stage approaches. Pseudomonas aeruginosa infections have a higher risk of infection relapse, with similar effectiveness of one- and two-stage strategies. B-hosts have a higher infection recurrence rate without comparable data between the two approaches. Further studies with a larger sample size are required to confirm our results and define B-hosts' best strategy.
Level of Evidence
Level III of evidence, retrospective cohort study investigating the results of treatments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


