Huamaní Charles , Concha-Velasco Fátima , Velásquez Lucio , K. Antich María , Cassa Johar , Palacios Kevin , Bernable-Villasante Luz , Giraldo-Alencastre Guido , Benites-Calderon Eduarda , Mendieta-Nuñez Sebastian , Quispe-Jihuallanca Heber , Quispe-Yana Matilde , Zavala-Vargas Karla , Hinojosa-Florez Liesbeth , Ramírez-Escobar Javier , Spelucin-Runciman Juan , Bernabe-Ortiz Antonio
{"title":"Differences in SARS-COV-2 seroprevalence in the population of Cusco, Peru","authors":"Huamaní Charles , Concha-Velasco Fátima , Velásquez Lucio , K. Antich María , Cassa Johar , Palacios Kevin , Bernable-Villasante Luz , Giraldo-Alencastre Guido , Benites-Calderon Eduarda , Mendieta-Nuñez Sebastian , Quispe-Jihuallanca Heber , Quispe-Yana Matilde , Zavala-Vargas Karla , Hinojosa-Florez Liesbeth , Ramírez-Escobar Javier , Spelucin-Runciman Juan , Bernabe-Ortiz Antonio","doi":"10.1016/j.gloepi.2023.100131","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>The spread of the coronavirus disease 2019 (COVID-19) in Peru has been reported at the regional level, few studies have evaluated its spread at the provincial level, in which the mechanisms could be different.</p></div><div><h3>Methods</h3><p>We conducted an analytical, cross-sectional, multistage observational population study to assess the seroprevalence of SARS-COV-2 at the provincial and urban/rural levels in a high-altitude setting. The sampling unit was the household, including a randomly selected family member. Sampling was performed using a data collection sheet on clinical and epidemiological variables. Chemiluminescence tests were used to detect total anti-SARS-COV-2 antibodies (IgG and IgM simultaneously). The percentages were adjusted to the sampling design.</p></div><div><h3>Results</h3><p>The overall prevalence in the region of Cusco was 25.9%, with considerably different prevalence between the 13 provinces (from 15.9% in Acomayo to 40.1% in Canchis) and between rural (21.1%) and urban (31.7%) areas. In multivariable model, living in a rural area was a protective factor (adjusted prevalence ratio [aPR], 0.68; 95% confidence interval [CI], 0.61–0.76).</p></div><div><h3>Conclusions</h3><p>Geographic diversity and population density determine different prevalence rates, typically lower in rural areas, possibly due to natural social distancing or limited interaction with people at risk.</p></div>","PeriodicalId":36311,"journal":{"name":"Global Epidemiology","volume":"7 ","pages":"Article 100131"},"PeriodicalIF":0.0000,"publicationDate":"2023-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2590113323000342/pdfft?md5=0d8eb9bd7d89e383599b818e3f7767de&pid=1-s2.0-S2590113323000342-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Epidemiology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590113323000342","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The spread of the coronavirus disease 2019 (COVID-19) in Peru has been reported at the regional level, few studies have evaluated its spread at the provincial level, in which the mechanisms could be different.
Methods
We conducted an analytical, cross-sectional, multistage observational population study to assess the seroprevalence of SARS-COV-2 at the provincial and urban/rural levels in a high-altitude setting. The sampling unit was the household, including a randomly selected family member. Sampling was performed using a data collection sheet on clinical and epidemiological variables. Chemiluminescence tests were used to detect total anti-SARS-COV-2 antibodies (IgG and IgM simultaneously). The percentages were adjusted to the sampling design.
Results
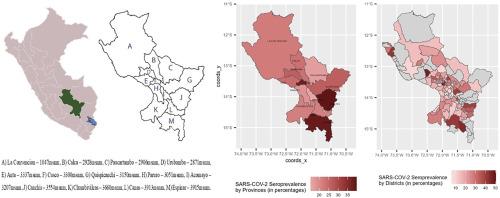
The overall prevalence in the region of Cusco was 25.9%, with considerably different prevalence between the 13 provinces (from 15.9% in Acomayo to 40.1% in Canchis) and between rural (21.1%) and urban (31.7%) areas. In multivariable model, living in a rural area was a protective factor (adjusted prevalence ratio [aPR], 0.68; 95% confidence interval [CI], 0.61–0.76).
Conclusions
Geographic diversity and population density determine different prevalence rates, typically lower in rural areas, possibly due to natural social distancing or limited interaction with people at risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


