{"title":"Serum soluble LYVE1 is a promising non-invasive biomarker of renal fibrosis: a population-based retrospective cross-sectional study.","authors":"Jing Liu, Yuqing Liu, Wenqian Zhou, Yiguo Liu, Saiya Zhu, Ying Yu, Jieli Huang, Chen Yu","doi":"10.1007/s12026-023-09448-3","DOIUrl":null,"url":null,"abstract":"<p><p>Diagnosis of renal fibrosis can only be verified by kidney biopsy, but biomarkers for non-invasive evaluation remain unsatisfactory. Patients with fibrosis often have abnormalities of the lymphatic vascular system and associated immune function. We describe here a lymphatic marker as a candidate biomarker for fibrosis. After assessing and grading the fibrosis scores, testing serum soluble lymphatic vessel endothelial hyaluronan receptor1 (sLYVE1) level, and collecting clinical information, the association between sLYVE1 and renal fibrosis was analyzed. Logistic regression analysis was used to screen variables. Diagnosis models with or without sLYVE1 were built, and nomograms were plotted. Calibration curve, C-index, and DCA were performed to assess the models. A total of 298 patients were enrolled in the study, of which 199 were included in the training cohort and 99 patients in the validation cohort. Serum sLYVE1 levels markedly elevated with increasing fibrosis grade (p<0.05). ROC analysis of sLYVE1 showed an AUC of 0.791 and 0.846 with optimal cut-off value of 405.25 ng/mL and 498.55 ng/mL for the prediction of moderate-to-severe renal fibrosis (MSF) and severe renal fibrosis (SF), respectively. The diagnostic nomogram model without sLYVE1 (model 1) included traditional clinical determinants (C-index: 0.658 for MSF; 0.603 for SF). A combination of model 1 and sLYVE1 (model 2) improved predictive performance (C-index: 0.847 for MSF; 0.856 for SF). Calibration curve and DCA demonstrated a better consistency accuracy and clinical benefit of model 2 than model 1. Serum sLYVE1 may be identified as a potential biomarker of renal fibrosis. Models incorporating sLYVE1 may be beneficial for a more accurate non-invasive diagnosis of renal fibrosis.</p>","PeriodicalId":3,"journal":{"name":"ACS Applied Electronic Materials","volume":null,"pages":null},"PeriodicalIF":4.3000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11217098/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Electronic Materials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12026-023-09448-3","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ENGINEERING, ELECTRICAL & ELECTRONIC","Score":null,"Total":0}
引用次数: 0
Abstract
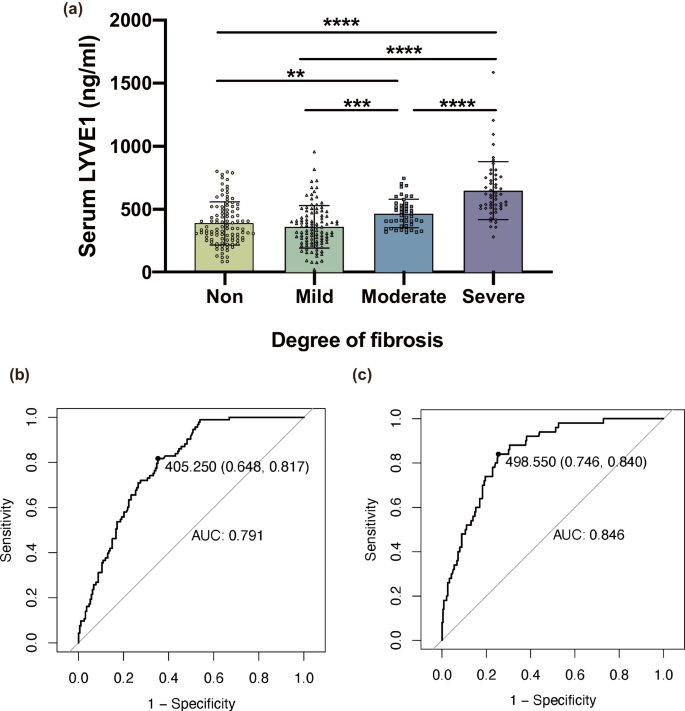
Diagnosis of renal fibrosis can only be verified by kidney biopsy, but biomarkers for non-invasive evaluation remain unsatisfactory. Patients with fibrosis often have abnormalities of the lymphatic vascular system and associated immune function. We describe here a lymphatic marker as a candidate biomarker for fibrosis. After assessing and grading the fibrosis scores, testing serum soluble lymphatic vessel endothelial hyaluronan receptor1 (sLYVE1) level, and collecting clinical information, the association between sLYVE1 and renal fibrosis was analyzed. Logistic regression analysis was used to screen variables. Diagnosis models with or without sLYVE1 were built, and nomograms were plotted. Calibration curve, C-index, and DCA were performed to assess the models. A total of 298 patients were enrolled in the study, of which 199 were included in the training cohort and 99 patients in the validation cohort. Serum sLYVE1 levels markedly elevated with increasing fibrosis grade (p<0.05). ROC analysis of sLYVE1 showed an AUC of 0.791 and 0.846 with optimal cut-off value of 405.25 ng/mL and 498.55 ng/mL for the prediction of moderate-to-severe renal fibrosis (MSF) and severe renal fibrosis (SF), respectively. The diagnostic nomogram model without sLYVE1 (model 1) included traditional clinical determinants (C-index: 0.658 for MSF; 0.603 for SF). A combination of model 1 and sLYVE1 (model 2) improved predictive performance (C-index: 0.847 for MSF; 0.856 for SF). Calibration curve and DCA demonstrated a better consistency accuracy and clinical benefit of model 2 than model 1. Serum sLYVE1 may be identified as a potential biomarker of renal fibrosis. Models incorporating sLYVE1 may be beneficial for a more accurate non-invasive diagnosis of renal fibrosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


