Christina K Chan, Mercedes Magaz, Victoria R Williams, Julie Wong, Monica Klein-Nouri, Sid Feldman, Jaclyn O'Brien, Natasha Salt, Andrew E Simor, Jocelyn Charles, Brian M Wong, Steve Shadowitz, Karen Fleming, Adrienne K Chan, Jerome A Leis
{"title":"Integration of hospital with congregate care homes in response to the COVID-19 pandemic.","authors":"Christina K Chan, Mercedes Magaz, Victoria R Williams, Julie Wong, Monica Klein-Nouri, Sid Feldman, Jaclyn O'Brien, Natasha Salt, Andrew E Simor, Jocelyn Charles, Brian M Wong, Steve Shadowitz, Karen Fleming, Adrienne K Chan, Jerome A Leis","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The coronavirus disease 2019 (COVID-19) pandemic has highlighted the need to improve the safety of the environments where we care for older adults in Canada. After providing assistance during the first wave, many Ontario hospitals formally partnered with local congregate care homes in a \"hub and spoke\" model during second pandemic wave onward. The objective of this article is to describe the implementation and longitudinal outcomes of residents in one hub and spoke model composed of a hospital partnered with 18 congregate care homes including four long-term care and 14 retirement or other congregate care homes.</p><p><strong>Intervention: </strong>Homes were provided continuous seven-day per week access to hospital support, including infection prevention and control (IPAC), testing, vaccine delivery and clinical support as needed. Any COVID-19 exposure or transmission triggered a same-day meeting to implement initial control measures. A minimum of weekly on-site visits occurred for long-term care homes and biweekly for other congregate care homes, with up to daily on-site presence during outbreaks.</p><p><strong>Outcomes: </strong>Case detection among residents increased following implementation in context of increased testing, then decreased post-immunization until the Omicron wave when it peaked. After adjusting for the correlation within homes, COVID-related mortality decreased following implementation (OR=0.51, 95% CI, 0.30-0.88; <i>p</i>=0.01). In secondary analysis, homes without pre-existing IPAC programs had higher baseline COVID-related mortality rate (OR=19.19, 95% CI, 4.66-79.02; <i>p</i><0.001) and saw a larger overall decrease during implementation (3.76% to 0.37%-0.98%) as compared to homes with pre-existing IPAC programs (0.21% to 0.57%-0.90%).</p><p><strong>Conclusion: </strong>The outcomes for older adults residing in congregate care homes improved steadily throughout the COVID-19 pandemic. While this finding is multifactorial, integration with a local hospital partner supported key interventions known to protect residents.</p>","PeriodicalId":94304,"journal":{"name":"Canada communicable disease report = Releve des maladies transmissibles au Canada","volume":"49 2-3","pages":"67-75"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10715829/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canada communicable disease report = Releve des maladies transmissibles au Canada","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The coronavirus disease 2019 (COVID-19) pandemic has highlighted the need to improve the safety of the environments where we care for older adults in Canada. After providing assistance during the first wave, many Ontario hospitals formally partnered with local congregate care homes in a "hub and spoke" model during second pandemic wave onward. The objective of this article is to describe the implementation and longitudinal outcomes of residents in one hub and spoke model composed of a hospital partnered with 18 congregate care homes including four long-term care and 14 retirement or other congregate care homes.
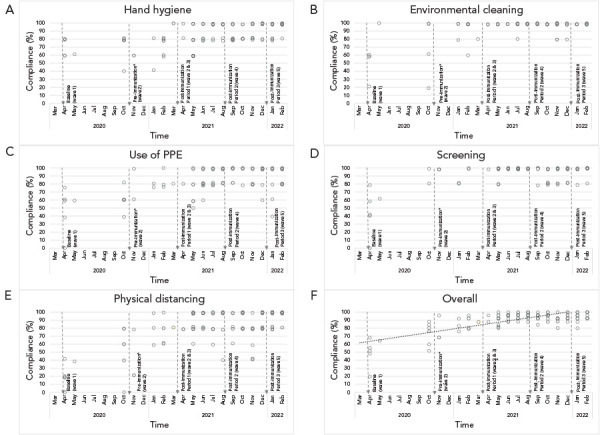
Intervention: Homes were provided continuous seven-day per week access to hospital support, including infection prevention and control (IPAC), testing, vaccine delivery and clinical support as needed. Any COVID-19 exposure or transmission triggered a same-day meeting to implement initial control measures. A minimum of weekly on-site visits occurred for long-term care homes and biweekly for other congregate care homes, with up to daily on-site presence during outbreaks.
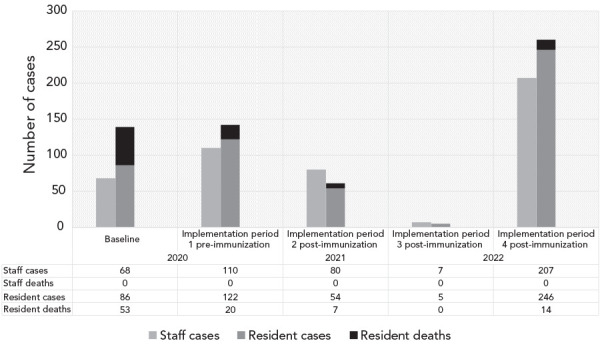
Outcomes: Case detection among residents increased following implementation in context of increased testing, then decreased post-immunization until the Omicron wave when it peaked. After adjusting for the correlation within homes, COVID-related mortality decreased following implementation (OR=0.51, 95% CI, 0.30-0.88; p=0.01). In secondary analysis, homes without pre-existing IPAC programs had higher baseline COVID-related mortality rate (OR=19.19, 95% CI, 4.66-79.02; p<0.001) and saw a larger overall decrease during implementation (3.76% to 0.37%-0.98%) as compared to homes with pre-existing IPAC programs (0.21% to 0.57%-0.90%).
Conclusion: The outcomes for older adults residing in congregate care homes improved steadily throughout the COVID-19 pandemic. While this finding is multifactorial, integration with a local hospital partner supported key interventions known to protect residents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


