Predicting 3-month Functional Outcome After Endovascular Thrombectomy in Patients with Anterior Circulation Occlusion with an Arterial Transit Artifact Grading System.
{"title":"Predicting 3-month Functional Outcome After Endovascular Thrombectomy in Patients with Anterior Circulation Occlusion with an Arterial Transit Artifact Grading System.","authors":"Xiaobo Zhang, Nannan Han, Yu Zhang, Wenting Yuan, Shangguang Kan, Gejuan Zhang, Haojun Ma, Hanming Ge, Chengxue Du, Yanjun Gao, Shilin Li, Xudong Yan, Wenzhen Shi, Ye Tian, Mingze Chang","doi":"10.1007/s00062-023-01362-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The objective of this study was to evaluate the relationship between arterial transit artifact (ATA), arterial spin labeling (ASL) perfusion imaging, and the outcome of patients with acute ischemic stroke (AIS) due to occlusion of large vessels in anterior circulation after endovascular thrombectomy (EVT).</p><p><strong>Methods: </strong>Patients with anterior circulation occlusion treated with EVT between October 2017 and December 2021 were enrolled in this retrospective study, and ATA was quantified by a 4-point scale. A favorable outcome was defined by modified Rankin Scale (mRS) scores of 0-2 at 3 months. To identify independent predictors of favorable outcome, age, sex, risk factors, baseline National Institutes of Health Stroke Scale (NIHSS) score, site of occlusion, cause of stroke, and early reperfusion were evaluated with univariate and multivariate analyses. Predictive accuracy was evaluated by calculating the area under the receiver operating characteristic (ROC) curve (AUC) for the model.</p><p><strong>Results: </strong>In this study 187 patients (age, 65.0 ± 12.5 years; men, 55%) were evaluated. Younger age (odds ratio, OR, 0.95; 95% confidence interval, CI, 0.92-0.98, p = 0.002), lower baseline NIHSS score (OR, 0.88; 95% CI, 0.82-0.94, p < 0.001), and lower ATA score (OR, 1.14; 95% CI, 1.06-1.22, p < 0.001) were independently associated with favorable outcomes in multivariate analysis. The ATA score has moderate to good accuracy in predicting favorable outcomes (AUC, 0.753).</p><p><strong>Conclusion: </strong>A high ATA score as a potential predictor, can help identify patients who may benefit from EVT.</p>","PeriodicalId":10391,"journal":{"name":"Clinical Neuroradiology","volume":" ","pages":"241-249"},"PeriodicalIF":2.8000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Neuroradiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00062-023-01362-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/5 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The objective of this study was to evaluate the relationship between arterial transit artifact (ATA), arterial spin labeling (ASL) perfusion imaging, and the outcome of patients with acute ischemic stroke (AIS) due to occlusion of large vessels in anterior circulation after endovascular thrombectomy (EVT).
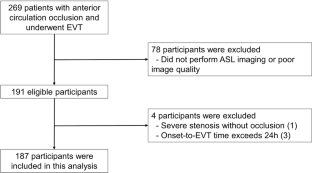
Methods: Patients with anterior circulation occlusion treated with EVT between October 2017 and December 2021 were enrolled in this retrospective study, and ATA was quantified by a 4-point scale. A favorable outcome was defined by modified Rankin Scale (mRS) scores of 0-2 at 3 months. To identify independent predictors of favorable outcome, age, sex, risk factors, baseline National Institutes of Health Stroke Scale (NIHSS) score, site of occlusion, cause of stroke, and early reperfusion were evaluated with univariate and multivariate analyses. Predictive accuracy was evaluated by calculating the area under the receiver operating characteristic (ROC) curve (AUC) for the model.
Results: In this study 187 patients (age, 65.0 ± 12.5 years; men, 55%) were evaluated. Younger age (odds ratio, OR, 0.95; 95% confidence interval, CI, 0.92-0.98, p = 0.002), lower baseline NIHSS score (OR, 0.88; 95% CI, 0.82-0.94, p < 0.001), and lower ATA score (OR, 1.14; 95% CI, 1.06-1.22, p < 0.001) were independently associated with favorable outcomes in multivariate analysis. The ATA score has moderate to good accuracy in predicting favorable outcomes (AUC, 0.753).
Conclusion: A high ATA score as a potential predictor, can help identify patients who may benefit from EVT.
期刊介绍:
Clinical Neuroradiology provides current information, original contributions, and reviews in the field of neuroradiology. An interdisciplinary approach is accomplished by diagnostic and therapeutic contributions related to associated subjects.
The international coverage and relevance of the journal is underlined by its being the official journal of the German, Swiss, and Austrian Societies of Neuroradiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


