Elevation of tacrolimus concentration after administration of methotrexate for treatment of graft-versus-host disease in pediatric patients received allogeneic hematopoietic stem cell transplantation.
{"title":"Elevation of tacrolimus concentration after administration of methotrexate for treatment of graft-versus-host disease in pediatric patients received allogeneic hematopoietic stem cell transplantation.","authors":"Chiaki Inoue, Takehito Yamamoto, Hiroshi Miyata, Hiroshi Suzuki, Tappei Takada","doi":"10.1186/s40780-023-00306-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Methotrexate (MTX) is used to treat graft-versus-host disease (GVHD) following allogeneic hematopoietic stem cell transplantation (allo-HSCT). Recently, a case was encountered in which the blood concentration of tacrolimus (TCR) at steady state increased after intravenous MTX administration for GVHD treatment (therapeutic IV-MTX administration). Therefore, this study aimed to investigate the effect of therapeutic IV-MTX administration on the pharmacokinetics of TCR.</p><p><strong>Methods: </strong>This single-center, retrospective, observational study included patients who underwent allo-HSCT and received therapeutic IV-MTX administration during immunosuppressive therapy with continuous intravenous infusion (CIV) of TCR from April 2004 to December 2021. Here, each therapeutic IV-MTX administration was defined as a case and independently subjected to subsequent analyses. The blood concentration of TCR at steady state (C<sub>ss</sub>), ratio of C<sub>ss</sub> to daily TCR dose (C/D), and clinical laboratory data were compared before and after therapeutic IV-MTX administration. In addition, dose changes in the TCR after therapeutic IV-MTX administration were evaluated.</p><p><strong>Results: </strong>Ten patients (23 cases) were included in this study. The C/D value significantly increased after therapeutic IV-MTX administration (median: 697 vs. 771 (ng/mL)/(mg/kg), 1.16-fold increase, P < 0.05), indicating a reduction in the apparent clearance of TCR. Along with the increase in C/D, significant increases were observed in aspartate transaminase level (median: 51.0 vs. 92.9 U/L, P < 0.01) and alanine aminotransferase level (median: 74.5 vs. 99.4 U/L, P < 0.01) indicating that liver injury after therapeutic IV-MTX administration contributes to the observed C/D increase. In addition, the daily dose of TCR was reduced in 11 cases (47.8%) after therapeutic IV-MTX administration, and the relative frequency of dose reduction tended to be higher than that of dose increase (median: 37.5% vs. 0.0%, P = 0.0519, permuted Brunner-Munzel test). The magnitude of dose reduction was 18.8% (7.4-50.0%) in the 11 cases with dose reduction.</p><p><strong>Conclusions: </strong>Therapeutic IV-MTX administration cause a significant increase in C/D, which requires TCR dose reduction. Careful therapeutic drug monitoring of TCR is needed after therapeutic IV-MTX administration in patients receiving immunosuppressive therapy with TCR after allo-HSCT.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"9 1","pages":"38"},"PeriodicalIF":1.2000,"publicationDate":"2023-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10696830/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-023-00306-w","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Methotrexate (MTX) is used to treat graft-versus-host disease (GVHD) following allogeneic hematopoietic stem cell transplantation (allo-HSCT). Recently, a case was encountered in which the blood concentration of tacrolimus (TCR) at steady state increased after intravenous MTX administration for GVHD treatment (therapeutic IV-MTX administration). Therefore, this study aimed to investigate the effect of therapeutic IV-MTX administration on the pharmacokinetics of TCR.
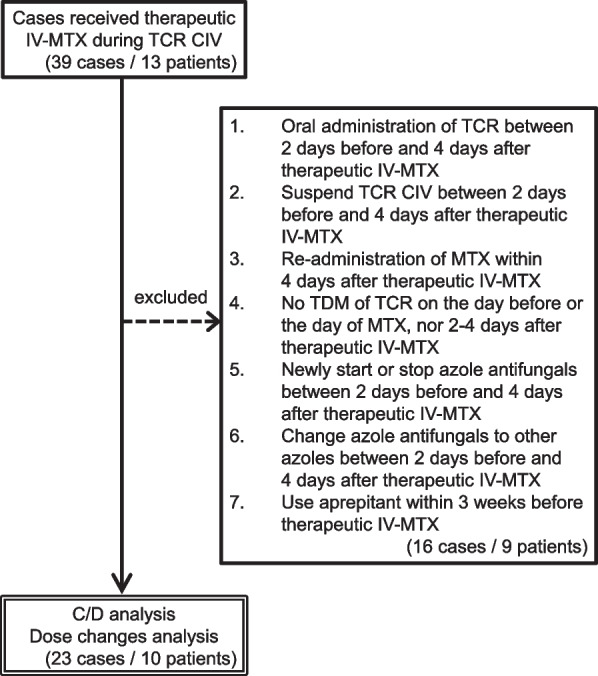
Methods: This single-center, retrospective, observational study included patients who underwent allo-HSCT and received therapeutic IV-MTX administration during immunosuppressive therapy with continuous intravenous infusion (CIV) of TCR from April 2004 to December 2021. Here, each therapeutic IV-MTX administration was defined as a case and independently subjected to subsequent analyses. The blood concentration of TCR at steady state (Css), ratio of Css to daily TCR dose (C/D), and clinical laboratory data were compared before and after therapeutic IV-MTX administration. In addition, dose changes in the TCR after therapeutic IV-MTX administration were evaluated.
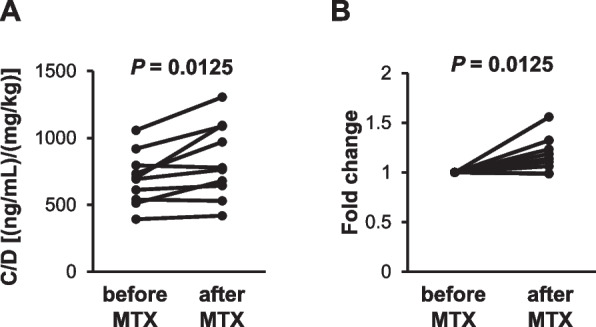
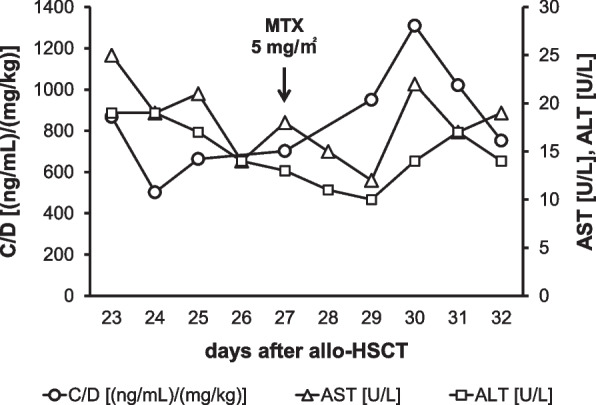
Results: Ten patients (23 cases) were included in this study. The C/D value significantly increased after therapeutic IV-MTX administration (median: 697 vs. 771 (ng/mL)/(mg/kg), 1.16-fold increase, P < 0.05), indicating a reduction in the apparent clearance of TCR. Along with the increase in C/D, significant increases were observed in aspartate transaminase level (median: 51.0 vs. 92.9 U/L, P < 0.01) and alanine aminotransferase level (median: 74.5 vs. 99.4 U/L, P < 0.01) indicating that liver injury after therapeutic IV-MTX administration contributes to the observed C/D increase. In addition, the daily dose of TCR was reduced in 11 cases (47.8%) after therapeutic IV-MTX administration, and the relative frequency of dose reduction tended to be higher than that of dose increase (median: 37.5% vs. 0.0%, P = 0.0519, permuted Brunner-Munzel test). The magnitude of dose reduction was 18.8% (7.4-50.0%) in the 11 cases with dose reduction.
Conclusions: Therapeutic IV-MTX administration cause a significant increase in C/D, which requires TCR dose reduction. Careful therapeutic drug monitoring of TCR is needed after therapeutic IV-MTX administration in patients receiving immunosuppressive therapy with TCR after allo-HSCT.
背景:甲氨蝶呤(MTX)用于治疗同种异体造血干细胞移植后的移植物抗宿主病(GVHD)。最近报道了一例静脉给药MTX治疗GVHD(治疗性IV-MTX给药)后他克莫司(TCR)稳态血药浓度升高的病例。因此,本研究旨在探讨IV-MTX治疗性给药对TCR药代动力学的影响。方法:这项单中心、回顾性、观察性研究纳入了2004年4月至2021年12月接受同种异体造血干细胞移植并在持续静脉输注TCR (CIV)免疫抑制治疗期间接受IV-MTX治疗的患者。在这里,每次IV-MTX治疗被定义为一个病例,并独立地进行后续分析。比较IV-MTX治疗前后TCR稳态血药浓度(Css)、Css与TCR日剂量之比(C/D)及临床实验室数据。此外,评估IV-MTX治疗后TCR的剂量变化。结果:10例患者(23例)纳入本研究。IV-MTX治疗性给药后C/D值显著升高(中位数:697 vs. 771 (ng/mL)/(mg/kg),增加1.16倍,P结论:IV-MTX治疗性给药导致C/D显著升高,需要减少TCR剂量。对于同种异体造血干细胞移植后接受TCR免疫抑制治疗的患者,在给予IV-MTX治疗性治疗后,需要仔细监测TCR。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


