Association between alcohol-associated cirrhosis and inpatient complications among COVID-19 patients: A propensity-matched analysis from the United States.
Faisal Inayat, Hassam Ali, Pratik Patel, Rubaid Dhillon, Arslan Afzal, Attiq Ur Rehman, Muhammad Sohaib Afzal, Laraib Zulfiqar, Gul Nawaz, Muhammad Hassan Naeem Goraya, Subanandhini Subramanium, Saurabh Agrawal, Sanjaya K Satapathy
{"title":"Association between alcohol-associated cirrhosis and inpatient complications among COVID-19 patients: A propensity-matched analysis from the United States.","authors":"Faisal Inayat, Hassam Ali, Pratik Patel, Rubaid Dhillon, Arslan Afzal, Attiq Ur Rehman, Muhammad Sohaib Afzal, Laraib Zulfiqar, Gul Nawaz, Muhammad Hassan Naeem Goraya, Subanandhini Subramanium, Saurabh Agrawal, Sanjaya K Satapathy","doi":"10.5501/wjv.v12.i4.221","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alcohol-associated cirrhosis (AC) contributes to significant liver-related mortality in the United States. It is known to cause immune dysfunction and coagulation abnormalities. Patients with comorbid conditions like AC are at risk of worse clinical outcomes from coronavirus disease 2019 (COVID-19). The specific association between AC and COVID-19 mortality remains inconclusive, given the lack of robust clinical evidence from prior studies.</p><p><strong>Aim: </strong>To study the predictors of mortality and the outcomes of AC in patients hospitalized with COVID-19 in the United States.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using the National Inpatient Sample (NIS) database 2020. Patients were identified with primary COVID-19 hospitalizations based on an underlying diagnosis of AC. A matched comparison cohort of COVID-19 patients without AC was identified after 1:N propensity score matching based on baseline sociodemographic characteristics and Elixhauser comorbidities. Primary outcomes included median length of stay, median inpatient charges, and in-hospital mortality. Secondary outcomes included a prevalence of systemic complications.</p><p><strong>Results: </strong>A total of 1325 COVID-19 patients with AC were matched to 1135 patients without AC. There was no difference in median length of stay and hospital charges in COVID-19 patients with AC compared to non-AC (<i>P</i> > 0.05). There was an increased prevalence of septic shock (5.7% <i>vs</i> 4.1%), ventricular fibrillation/ventricular flutter (0.4% <i>vs</i> 0%), atrial fibrillation (13.2% <i>vs</i> 8.8%), atrial flutter (8.7% <i>vs</i> 4.4%), first-degree atrioventricular nodal block (0.8% <i>vs</i> 0%), upper extremity venous thromboembolism (1.5% <i>vs</i> 0%), and variceal bleeding (3.8% <i>vs</i> 0%) in the AC cohort compared to the non-AC cohort (<i>P</i> < 0.05). There was no difference in inpatient mortality in COVID-19 patients with non-AC compared to AC, with an odds ratio of 0.97 (95% confidence interval: 0.78-1.22, <i>P</i> = 0.85). Predictors of mortality included advanced age, cardiac arrhythmias, coagulopathy, protein-calorie malnutrition, fluid and electrolyte disorders, septic shock, and upper extremity venous thromboembolism.</p><p><strong>Conclusion: </strong>AC does not increase mortality in patients hospitalized with COVID-19. There is an increased association between inpatient complications among COVID-19 patients with AC compared to non-AC.</p>","PeriodicalId":61903,"journal":{"name":"世界病毒学杂志(英文版)","volume":"12 4","pages":"221-232"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10642379/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界病毒学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5501/wjv.v12.i4.221","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Alcohol-associated cirrhosis (AC) contributes to significant liver-related mortality in the United States. It is known to cause immune dysfunction and coagulation abnormalities. Patients with comorbid conditions like AC are at risk of worse clinical outcomes from coronavirus disease 2019 (COVID-19). The specific association between AC and COVID-19 mortality remains inconclusive, given the lack of robust clinical evidence from prior studies.
Aim: To study the predictors of mortality and the outcomes of AC in patients hospitalized with COVID-19 in the United States.
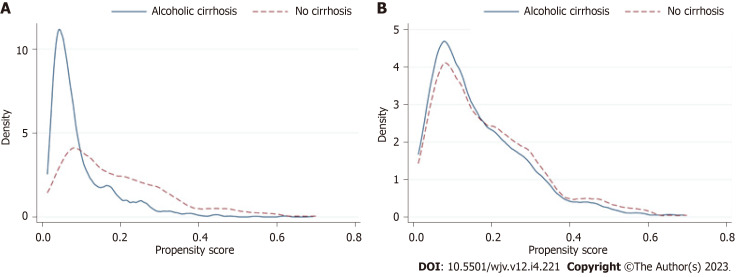
Methods: We conducted a retrospective cohort study using the National Inpatient Sample (NIS) database 2020. Patients were identified with primary COVID-19 hospitalizations based on an underlying diagnosis of AC. A matched comparison cohort of COVID-19 patients without AC was identified after 1:N propensity score matching based on baseline sociodemographic characteristics and Elixhauser comorbidities. Primary outcomes included median length of stay, median inpatient charges, and in-hospital mortality. Secondary outcomes included a prevalence of systemic complications.
Results: A total of 1325 COVID-19 patients with AC were matched to 1135 patients without AC. There was no difference in median length of stay and hospital charges in COVID-19 patients with AC compared to non-AC (P > 0.05). There was an increased prevalence of septic shock (5.7% vs 4.1%), ventricular fibrillation/ventricular flutter (0.4% vs 0%), atrial fibrillation (13.2% vs 8.8%), atrial flutter (8.7% vs 4.4%), first-degree atrioventricular nodal block (0.8% vs 0%), upper extremity venous thromboembolism (1.5% vs 0%), and variceal bleeding (3.8% vs 0%) in the AC cohort compared to the non-AC cohort (P < 0.05). There was no difference in inpatient mortality in COVID-19 patients with non-AC compared to AC, with an odds ratio of 0.97 (95% confidence interval: 0.78-1.22, P = 0.85). Predictors of mortality included advanced age, cardiac arrhythmias, coagulopathy, protein-calorie malnutrition, fluid and electrolyte disorders, septic shock, and upper extremity venous thromboembolism.
Conclusion: AC does not increase mortality in patients hospitalized with COVID-19. There is an increased association between inpatient complications among COVID-19 patients with AC compared to non-AC.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


