{"title":"Preventive plasmapheresis for rituximab related flare in cryoglobulinemic vasculitis","authors":"Léa Fornero , Tarik Kanouni , Jean-Jacques Tudesq , Camille Pochard , Pauline Verot , Wendy Renier , Ludovic Gabellier , Guillaume Cartron , Philippe Guilpain , Charles Herbaux","doi":"10.1016/j.jtauto.2023.100194","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>Rituximab monotherapy represents the main therapeutic option for cryoglobulinemic vasculitis (CV) with severe organ involvement. However, initial worsening of the CV, known as rituximab-associated CV flare (=CV flare), has been described and are associated with high mortality rates. The aim of the present study is to evaluate the outcomes of plasmapheresis initiated before or during rituximab treatment, as prevention of CV flare.</p></div><div><h3>Methods</h3><p>We conducted a retrospecttive study in our tertiary referral center from 2001 to 2020. We have included all patients with CV receiving rituximab and divided them in two groups whether they had flare prevention by plasmapheresis or not. We evaluated rituximab-related CV flare incidence in both groups. CV flare was defined as the onset of a new organ involvement or worsening of the initial manifestations within 4 weeks following rituximab.</p></div><div><h3>Results</h3><p>Among the 71 patients included, 44 received rituximab without plasmapheresis (control = CT cohort) and 27 received plasmapheresis before or during rituximab treatment (preventive plasmapheresis = PP cohort). PP was given to patients thought to have a high risk of CV flare, with significantly more severe diseases than patients in the CT cohort. Despite this, no CV flare was observed in the PP group. In the other hand, 5 flares occurred in the CT cohort.</p></div><div><h3>Conclusion</h3><p>Our results show that plasmapheresis is efficient and well tolerated to prevent rituximab-associated CV flare. We believe that our data support the use of plasmapheresis in this indication, especially in patients with high risk of CV flare.</p></div>","PeriodicalId":36425,"journal":{"name":"Journal of Translational Autoimmunity","volume":"6 ","pages":"Article 100194"},"PeriodicalIF":4.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9975310/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Translational Autoimmunity","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589909023000072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction
Rituximab monotherapy represents the main therapeutic option for cryoglobulinemic vasculitis (CV) with severe organ involvement. However, initial worsening of the CV, known as rituximab-associated CV flare (=CV flare), has been described and are associated with high mortality rates. The aim of the present study is to evaluate the outcomes of plasmapheresis initiated before or during rituximab treatment, as prevention of CV flare.
Methods
We conducted a retrospecttive study in our tertiary referral center from 2001 to 2020. We have included all patients with CV receiving rituximab and divided them in two groups whether they had flare prevention by plasmapheresis or not. We evaluated rituximab-related CV flare incidence in both groups. CV flare was defined as the onset of a new organ involvement or worsening of the initial manifestations within 4 weeks following rituximab.
Results
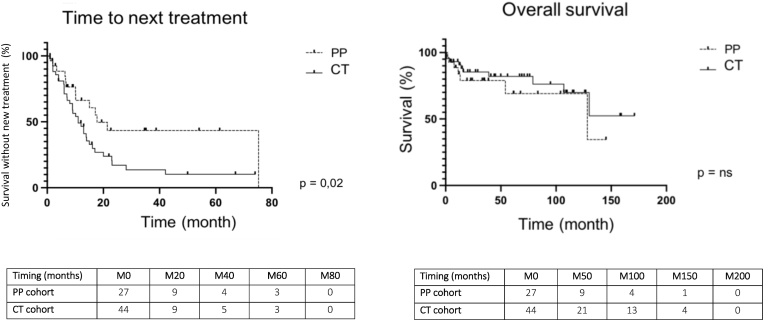
Among the 71 patients included, 44 received rituximab without plasmapheresis (control = CT cohort) and 27 received plasmapheresis before or during rituximab treatment (preventive plasmapheresis = PP cohort). PP was given to patients thought to have a high risk of CV flare, with significantly more severe diseases than patients in the CT cohort. Despite this, no CV flare was observed in the PP group. In the other hand, 5 flares occurred in the CT cohort.
Conclusion
Our results show that plasmapheresis is efficient and well tolerated to prevent rituximab-associated CV flare. We believe that our data support the use of plasmapheresis in this indication, especially in patients with high risk of CV flare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


