{"title":"Early Onset Outlet Obstruction of a Temporary Diverting Loop Ileostomy Secondary to Urinary Retention.","authors":"Umut Akova, Volkan Dogru, Eren Esen, Feza Remzi","doi":"10.1159/000529481","DOIUrl":null,"url":null,"abstract":"<p><p>A mechanical obstruction is not a physiological entity, and when it occurs within the 30-day postoperative period, it is called an early postoperative small bowel obstruction. Kinking of small bowel segments at the ileostomy outlet secondary to a distended bladder is an unusual source of early postoperative small bowel obstruction. A 36-year-old female underwent a redo J-Pouch surgery and creation of loop ileostomy after pouch failure related to recurrent small bowel obstruction and perianal fistulae. Her foley catheter was removed on postoperative day 3 and she passed a trial of void test. On postoperative day 6, the abdomen became progressively more distended. Computerized tomography (CT) imaging with IV contrast showed small bowel distension extending to the midline anterior to the urinary bladder where it demonstrated a narrowed lumen. These findings were thought to be the cause of small bowel obstruction at this level before the ileostomy. Immediately after CT, a foley catheter was applied with which 2 L of urine was removed, and consequently, gas and stool were observed in the ostomy soon thereafter. Although rare, urinary retention may cause intestinal obstruction, especially in the presence of a loop ileostomy in close proximity.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"17 1","pages":"124-128"},"PeriodicalIF":0.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/39/4d/crg-2023-0017-0001-529481.PMC9947664.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000529481","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
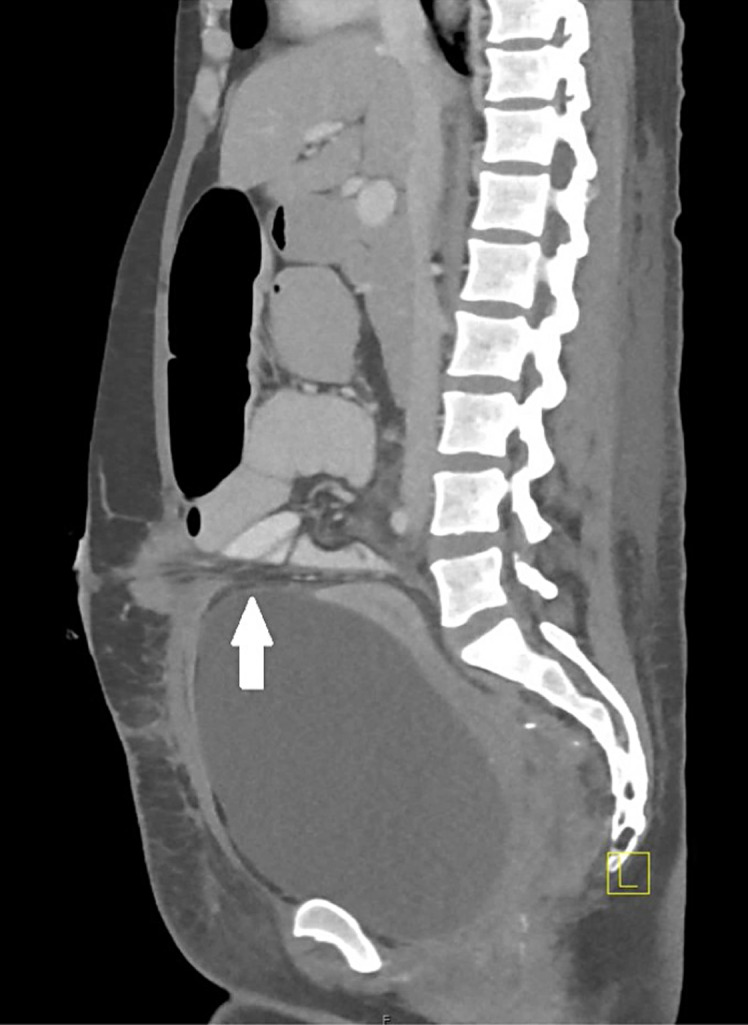
A mechanical obstruction is not a physiological entity, and when it occurs within the 30-day postoperative period, it is called an early postoperative small bowel obstruction. Kinking of small bowel segments at the ileostomy outlet secondary to a distended bladder is an unusual source of early postoperative small bowel obstruction. A 36-year-old female underwent a redo J-Pouch surgery and creation of loop ileostomy after pouch failure related to recurrent small bowel obstruction and perianal fistulae. Her foley catheter was removed on postoperative day 3 and she passed a trial of void test. On postoperative day 6, the abdomen became progressively more distended. Computerized tomography (CT) imaging with IV contrast showed small bowel distension extending to the midline anterior to the urinary bladder where it demonstrated a narrowed lumen. These findings were thought to be the cause of small bowel obstruction at this level before the ileostomy. Immediately after CT, a foley catheter was applied with which 2 L of urine was removed, and consequently, gas and stool were observed in the ostomy soon thereafter. Although rare, urinary retention may cause intestinal obstruction, especially in the presence of a loop ileostomy in close proximity.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


