{"title":"Prediction of white-coat hypertension and white-coat uncontrolled hypertension using machine learning algorithm.","authors":"Ling-Chieh Shih, Yu-Ching Wang, Ming-Hui Hung, Han Cheng, Yu-Chieh Shiao, Yu-Hsuan Tseng, Chin-Chou Huang, Shing-Jong Lin, Jaw-Wen Chen","doi":"10.1093/ehjdh/ztac066","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The detection of white-coat hypertension/white-coat uncontrolled hypertension (WCH/WUCH) with out-of-office blood pressure (BP) monitoring is time- and resource-consuming. We aim to develop a machine learning (ML)-derived prediction model based on the characteristics of patients from a single outpatient visit.</p><p><strong>Methods and results: </strong>Data from two cohorts in Taiwan were used. Cohort one (970 patients) was used for development and internal validation, and cohort two (464 patients) was used for external validation. WCH/WUCH was defined as an office BP of ≥140/90 mmHg and daytime ambulatory BP of <135/85 mmHg in treatment-naïve or treated individuals. Logistic regression, random forest (RF), eXtreme Gradient Boosting, and artificial neural network models were trained using 26 patient parameters. We used SHapley Additive exPlanations values to provide explanations for the risk factors. All models achieved great area under the receiver operating characteristic curve (AUROC), specificity, and negative predictive value in both validations (AUROC = 0.754-0.891; specificity = 0.682-0.910; negative predictive value = 0.831-0.968). The RF model was the best performing (AUROC = 0.884; sensitivity = 0.619; specificity = 0.887; negative predictive value = 0.872; accuracy = 0.819). The five most influential features of the RF model were office diastolic BP, office systolic BP, current smoker, estimated glomerular filtration rate, and fasting glucose level.</p><p><strong>Conclusion: </strong>Our prediction models achieved good performance, underlining the feasibility of applying ML models to outpatient populations for the diagnosis of WCH and WUCH. Further validation with other prospective data sets should be considered in the future.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"3 4","pages":"559-569"},"PeriodicalIF":3.9000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/0b/ztac066.PMC9779877.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztac066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Aims: The detection of white-coat hypertension/white-coat uncontrolled hypertension (WCH/WUCH) with out-of-office blood pressure (BP) monitoring is time- and resource-consuming. We aim to develop a machine learning (ML)-derived prediction model based on the characteristics of patients from a single outpatient visit.
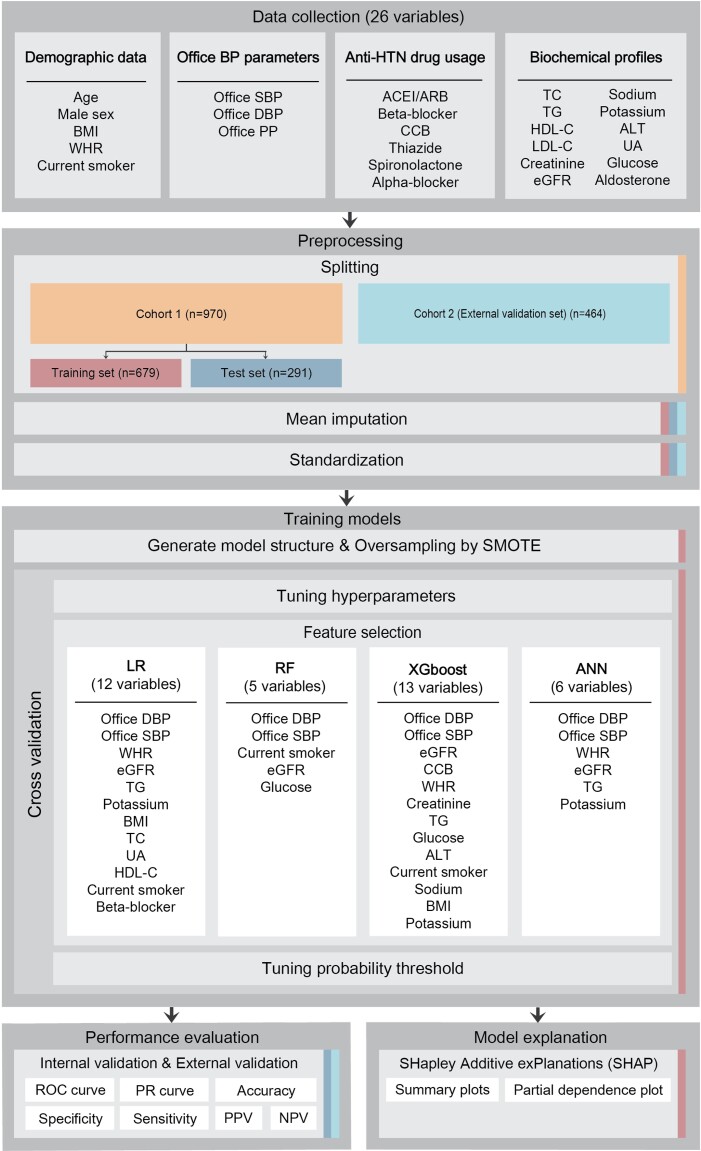
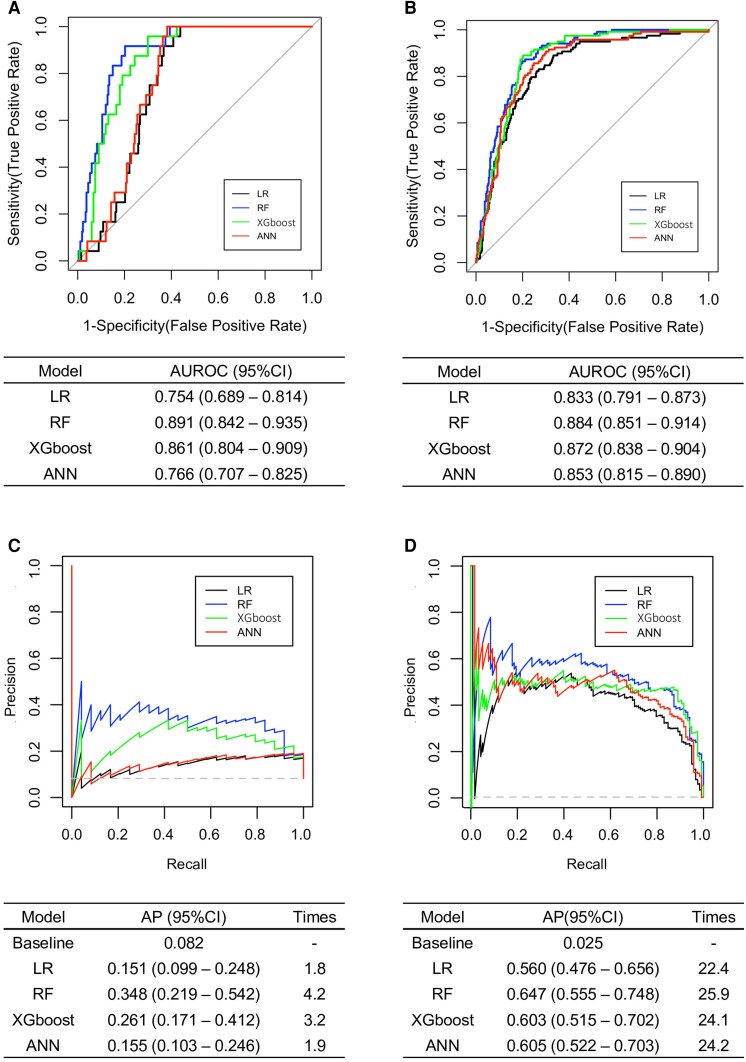
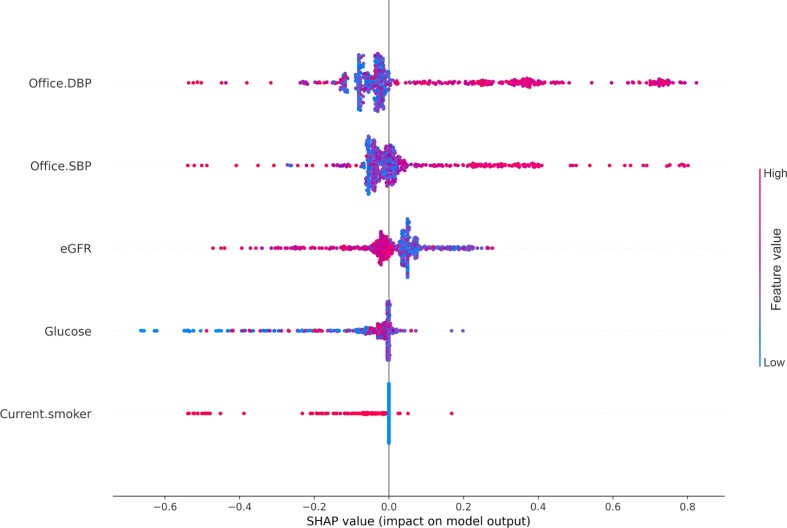
Methods and results: Data from two cohorts in Taiwan were used. Cohort one (970 patients) was used for development and internal validation, and cohort two (464 patients) was used for external validation. WCH/WUCH was defined as an office BP of ≥140/90 mmHg and daytime ambulatory BP of <135/85 mmHg in treatment-naïve or treated individuals. Logistic regression, random forest (RF), eXtreme Gradient Boosting, and artificial neural network models were trained using 26 patient parameters. We used SHapley Additive exPlanations values to provide explanations for the risk factors. All models achieved great area under the receiver operating characteristic curve (AUROC), specificity, and negative predictive value in both validations (AUROC = 0.754-0.891; specificity = 0.682-0.910; negative predictive value = 0.831-0.968). The RF model was the best performing (AUROC = 0.884; sensitivity = 0.619; specificity = 0.887; negative predictive value = 0.872; accuracy = 0.819). The five most influential features of the RF model were office diastolic BP, office systolic BP, current smoker, estimated glomerular filtration rate, and fasting glucose level.
Conclusion: Our prediction models achieved good performance, underlining the feasibility of applying ML models to outpatient populations for the diagnosis of WCH and WUCH. Further validation with other prospective data sets should be considered in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


