{"title":"Ipsilateral Limb Extension of Referred Trigeminal Facial Pain due to Greater Occipital Nerve Entrapment: A Case Report.","authors":"Byung-Chul Son, Changik Lee","doi":"10.1155/2022/9381881","DOIUrl":null,"url":null,"abstract":"<p><p>We report a very rare case of referred pain associated with entrapment of the greater occipital nerve (GON) occurring not only in the ipsilateral hemiface but also in the ipsilateral limb. There is an extensive convergence of cutaneous, tooth pulp, visceral, neck, and muscle afferents onto nociceptive and nonnociceptive neurons in the trigeminal nucleus caudalis (medullary dorsal horn). In addition, nociceptive input from trigeminal, meningeal afferents projects into trigeminal nucleus caudalis and dorsal horn of C1 and C2. Together, they form a functional unit, the trigeminocervical complex (TCC). The nociceptive inflow from suboccipital and high cervical structures is mediated with small-diameter afferent fibers in the upper cervical roots terminating in the dorsal horn of the cervical cord extending from the C2 segment up to the medullary dorsal horn. The major afferent contribution is mediated by the spinal root C2 that is peripherally represented by the greater occipital nerve (GON). Convergence of afferent signals from the trigeminal nerve and the GON onto the TCC is regarded as an anatomical basis of pain referral in craniofacial pain and primary headache syndrome. Ipsilateral limb pain occurs long before the onset of the referred facial pain. The subsequent severe hemifacial pain suggested GON entrapment. The occipital nerve block provided temporary relief from facial and extremity pain. Imaging studies found a benign osteoma in the ipsilateral suboccipital bone, but no direct contact with GON was identified. During GON decompression, severe entrapment of the GON was observed by the tendinous aponeurotic edge of the trapezius muscle, but the osteoma had no contact with the nerve. Following GON decompression, the referred trigeminal and extremity pain completely disappeared. The pain referral from GON entrapment seems to be attributed to the sensitization and hypersensitivity of the trigeminocervical complex (TCC). The clinical manifestations of TCC hypersensitivity induced by chronic entrapment of GONs are diverse when considering the occurrence of extremity pain as well as facial pain.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2022 ","pages":"9381881"},"PeriodicalIF":0.9000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9734007/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/9381881","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
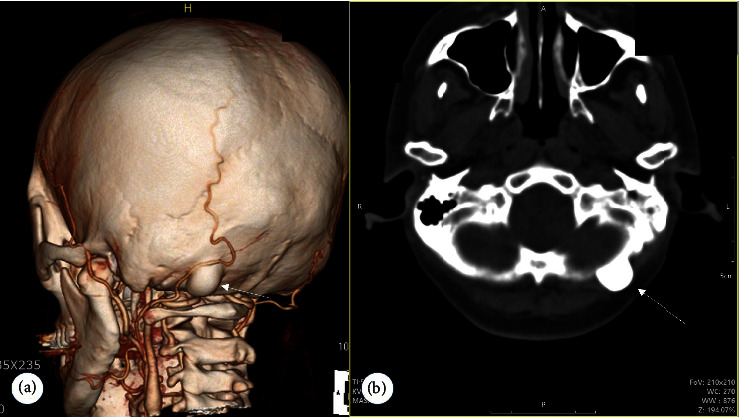
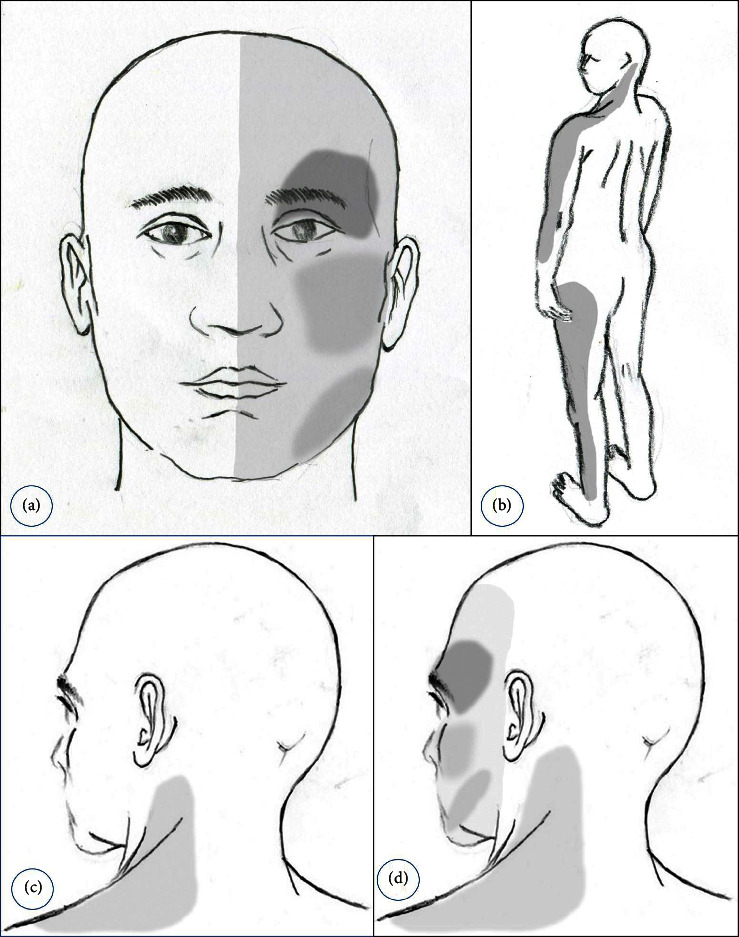
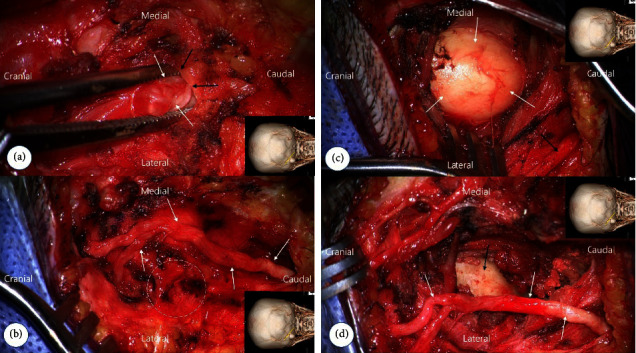
We report a very rare case of referred pain associated with entrapment of the greater occipital nerve (GON) occurring not only in the ipsilateral hemiface but also in the ipsilateral limb. There is an extensive convergence of cutaneous, tooth pulp, visceral, neck, and muscle afferents onto nociceptive and nonnociceptive neurons in the trigeminal nucleus caudalis (medullary dorsal horn). In addition, nociceptive input from trigeminal, meningeal afferents projects into trigeminal nucleus caudalis and dorsal horn of C1 and C2. Together, they form a functional unit, the trigeminocervical complex (TCC). The nociceptive inflow from suboccipital and high cervical structures is mediated with small-diameter afferent fibers in the upper cervical roots terminating in the dorsal horn of the cervical cord extending from the C2 segment up to the medullary dorsal horn. The major afferent contribution is mediated by the spinal root C2 that is peripherally represented by the greater occipital nerve (GON). Convergence of afferent signals from the trigeminal nerve and the GON onto the TCC is regarded as an anatomical basis of pain referral in craniofacial pain and primary headache syndrome. Ipsilateral limb pain occurs long before the onset of the referred facial pain. The subsequent severe hemifacial pain suggested GON entrapment. The occipital nerve block provided temporary relief from facial and extremity pain. Imaging studies found a benign osteoma in the ipsilateral suboccipital bone, but no direct contact with GON was identified. During GON decompression, severe entrapment of the GON was observed by the tendinous aponeurotic edge of the trapezius muscle, but the osteoma had no contact with the nerve. Following GON decompression, the referred trigeminal and extremity pain completely disappeared. The pain referral from GON entrapment seems to be attributed to the sensitization and hypersensitivity of the trigeminocervical complex (TCC). The clinical manifestations of TCC hypersensitivity induced by chronic entrapment of GONs are diverse when considering the occurrence of extremity pain as well as facial pain.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


