Shamsi Ghaffari, Khosro Hashemzadeh, Mahmood Samadi, Akbar Molaei, Sahar Sadeghi, Ahmad Jamei Khosroshahi
{"title":"Upward spontaneous migration of ventriculoperitoneal shunt into the heart: A case report summary.","authors":"Shamsi Ghaffari, Khosro Hashemzadeh, Mahmood Samadi, Akbar Molaei, Sahar Sadeghi, Ahmad Jamei Khosroshahi","doi":"10.34172/jcvtr.2022.30523","DOIUrl":null,"url":null,"abstract":"<p><p>A male infant with a history of ventriculoperitoneal (VP) implantation due to congenital hydrocephalus presented with fever and lethargy at the age of 8 month-old. Pericardial effusion was detected in transthoracic echocardiography, and he underwent pericardial window operation and was discharged in a stable condition. At 11 months of age, he presented again with fever, lethargy, recurrent vomiting, and respiratory distress. In both plain chest radiography and transthoracic echocardiography, VP shunt migration to the heart cavity was observed. The VP shunt had entered into the right ventricle after perforating the diaphragm and pericardium. The patient underwent open-heart surgery due to vegetation at the tip of the VP shunt inside the right heart. Vegetation was removed and the tip of the shunt was returned to the peritoneal cavity. Two weeks after discharge, the patient presented again with symptoms of tachypnea and lethargy. The imaging revealed the entry of the VP shunt about two centimeters into the anterior mediastinum. The patient was transferred to the operation room and the VP shunt was shortened and re-inserted into the peritoneal cavity. Antibiotic treatment was continued for six weeks and the patient was discharged in stable condition. In follow-up visits after two years, the VP shunt functioned well and no particular complication was observed. This case demonstrates that in patients with VP shunt implantation presenting with pulmonary and cardiac symptoms such as respiratory distress, pericardial effusion, and cardiac tamponade after VP shunt implantation, the possibility of VP shunt catheter migration to the mediastinal cavity should be considered.</p>","PeriodicalId":15207,"journal":{"name":"Journal of Cardiovascular and Thoracic Research","volume":"14 4","pages":"263-267"},"PeriodicalIF":1.2000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9871159/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular and Thoracic Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34172/jcvtr.2022.30523","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
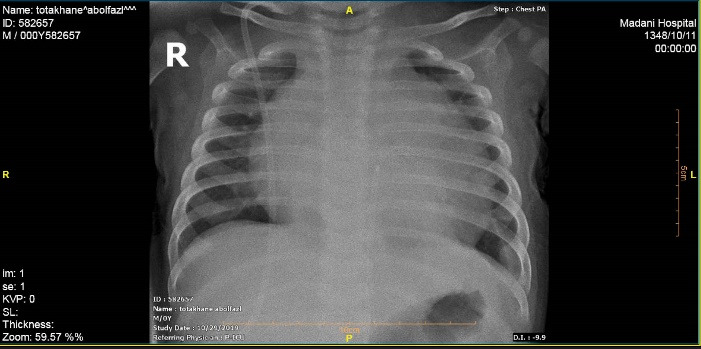
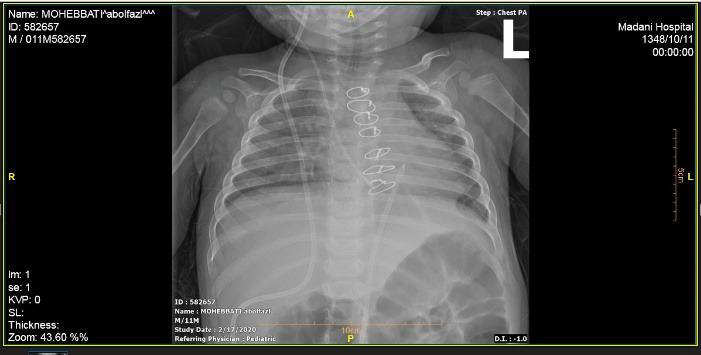
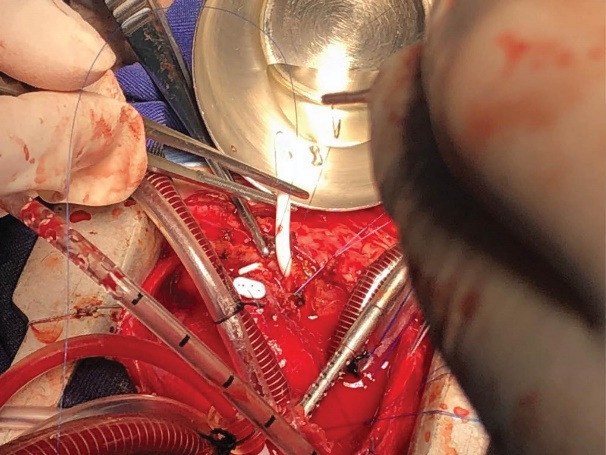
A male infant with a history of ventriculoperitoneal (VP) implantation due to congenital hydrocephalus presented with fever and lethargy at the age of 8 month-old. Pericardial effusion was detected in transthoracic echocardiography, and he underwent pericardial window operation and was discharged in a stable condition. At 11 months of age, he presented again with fever, lethargy, recurrent vomiting, and respiratory distress. In both plain chest radiography and transthoracic echocardiography, VP shunt migration to the heart cavity was observed. The VP shunt had entered into the right ventricle after perforating the diaphragm and pericardium. The patient underwent open-heart surgery due to vegetation at the tip of the VP shunt inside the right heart. Vegetation was removed and the tip of the shunt was returned to the peritoneal cavity. Two weeks after discharge, the patient presented again with symptoms of tachypnea and lethargy. The imaging revealed the entry of the VP shunt about two centimeters into the anterior mediastinum. The patient was transferred to the operation room and the VP shunt was shortened and re-inserted into the peritoneal cavity. Antibiotic treatment was continued for six weeks and the patient was discharged in stable condition. In follow-up visits after two years, the VP shunt functioned well and no particular complication was observed. This case demonstrates that in patients with VP shunt implantation presenting with pulmonary and cardiac symptoms such as respiratory distress, pericardial effusion, and cardiac tamponade after VP shunt implantation, the possibility of VP shunt catheter migration to the mediastinal cavity should be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


