Temporal Bone Imaging Opportunities With Ultra-High-Resolution Computed Tomography.
IF 1.1
Q3 OTORHINOLARYNGOLOGY
引用次数: 2
Abstract
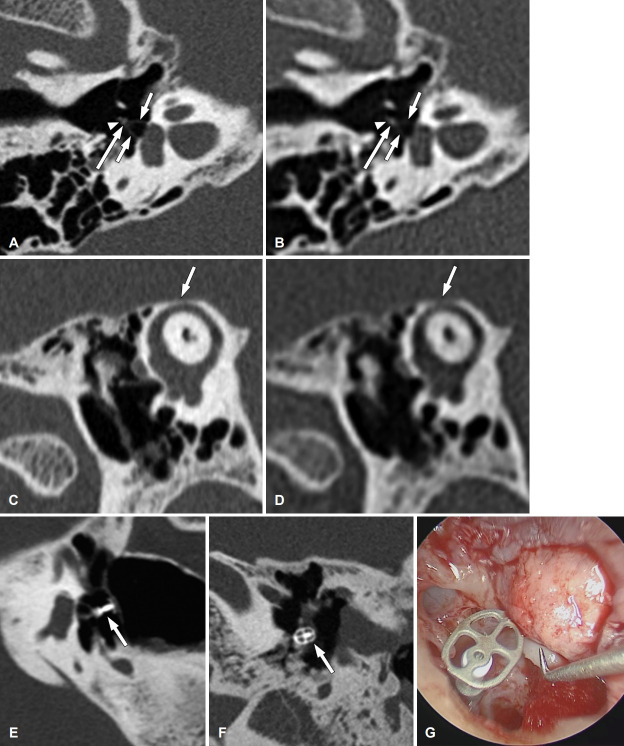
Dear Editor, Ultra-high-resolution computed tomography (U-HRCT) is an emerging technology that has been recently introduced in the clinical setting. It offers more spatial resolution than conventional multidetector-row computed tomography (MDCT), demonstrating substantial potential for improving clinical imaging. The main advantages of U-HRCT scanners include smaller detector elements and focus size, more channels and detector rows, and a higher matrix display than MDCT scanners. These features enable U-HRCT to improve spatial resolution from nearly 400-450 μm to approximately 150-200 μm, the width of a human hair [1,2]. Particularly, U-HRCT exhibits considerable potential in temporal bone imaging because of its complex anatomy with submillimeter structures, often requiring optimal multiplanar reconstructions with a high degree of spatial resolution. In the last few years, several publications have demonstrated that UHRCT considerably enhances the identification of small temporal bone structures compared to MDCT, such as the cochlea, incudostapedial joint, stapes footplate, stapedial muscle, and chorda tympani nerve (Fig. 1A and B) [1,3,4]. The anatomical information gained with U-HRCT may aid in the assessment of diseases of the middle and inner ear, such as otosclerosis and superior semicircular canal dehiscence (Fig. 1C and D). In otologic surgery, it may help to optimize patient selection, individualize surgical techniques, and improve postoperative evaluation [5]. Furthermore, the reduction of both “blooming” artifacts (from metallic materials) and partial volume effect gained with U-HRCT is especially beneficial for the precise evaluation of the position of metallic auditory implants (Fig. 1E-G), such as intravestibular stapes prosthesis protrusion and intracochlear electrode array position [6,7]. Recently, Heutink, et al. [8] reported the first in vivo detection of cochlear neo-ossification after cochlear implantation using U-HRCT, which had been previously described only on postmortem examination. U-HRCT has some inherent challenges. The increased spatial resolution has the downside of either an increase in image noise or an increase in radiation dosage to maintain the same levels of image noise. As a result, noise-reduction strategies become essential, including optimized image acquisition protocols and improved iterative reconstruction techniques. By reducing image noise, these reconstruction techniques allow for substantial radiation dose reduction while preserving image quality [9]. In addition, as spatial resolution increases and slice thickness reduces, the number of slices that must be interpreted will increase considerably. This significant rise in data volume will necessitate greater workstation post-processing power, faster network speeds, and more clinical server storage space [7]. In conclusion, U-HRCT is a commercially available technological advancement that offers higher quality images than conventional computed tomography. Despite increased image noise, U-HRCT enables sharper and more distinct images of the temporal bone, which may allow more accurate visualization of anatomic landmarks, improved disease detection (particularly subtle abnormalities), and optimized preoperative and postoperative evaluation. Successive improvements in noise-reduction strategies will have the potential to positively impact image quality, thereby allowing for radiation exposure reduction. As advances in temporal bone CT continue to expand, future studies will be needed to comprehensively evaluate their impact on clinical practice. Temporal Bone Imaging Opportunities With Ultra-High-Resolution Computed Tomography
超高分辨率计算机断层扫描颞骨成像的机会。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Journal of Audiology and Otology
OTORHINOLARYNGOLOGY-
CiteScore
1.90
自引率
9.10%
发文量
20
期刊介绍:
Journal of Audiology and Otology (JAO) (formerly known as Korean Journal of Audiology) aims to publish the most advanced findings for all aspects of the auditory and vestibular system and diseases of the ear using state-of-the-art techniques and analyses. The journal covers recent trends related to the topics of audiology, otology, and neurotology conducted by professionals, with the goal of providing better possible treatment to people of all ages, from infants to the elderly, who suffer from auditory and/or vestibular disorders and thus, improving their quality of life. This journal encourages the submission of review papers about current professional issues, research papers presenting a scientific base and clinical application, and case papers with unique reports or clinical trials. We also invite letters to the editor and papers related to the manufacture and distribution of medical devices. This journal provides integrated views from otologists, audiologists, and other healthcare practitioners, offering readers high quality scientific and clinical information. This peer-reviewed and open access journal has been the official journal of the Korean Audiological Society since 1997 and of both the Korean Audiological Society and the Korean Otological Society since 2017. It is published in English four times a year in January, April, July, and October.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


