Venkata Vinod Kumar Matli, David F Dies, Sudha Pandit, Gregory Wellman, James D Morris
{"title":"Distinction between Mitochondrial Antibody-Positive and -Negative Primary Biliary Cholangitis.","authors":"Venkata Vinod Kumar Matli, David F Dies, Sudha Pandit, Gregory Wellman, James D Morris","doi":"10.1159/000528437","DOIUrl":null,"url":null,"abstract":"<p><p>Antimitochondrial antibody-positive primary biliary cholangitis (AMA-pos PBC) is an autoimmune disorder in which monoclonal antibodies are produced against epitopes in the mitochondrial membranes of biliary epithelial cells, resulting in progressive nonsuppurative biliary cholangitis. Up to 5% of patients lack these autoantibodies, termed antimitochondrial antibody-negative (AMA-neg) PBC. Although a somewhat new variant of AMA-pos PBC, it is not an overlapping syndrome. Few studies to date have described this phenomenon. An 87-year-old woman was referred to our clinic with elevated serum alkaline phosphatase (714 U/L). She reported fatigue but no other symptoms. A physical examination revealed a benign lesion and bilateral lower extremity swelling secondary to lymphedema. The serological profile was significant for a high antinuclear antibody titer (>1:2,560) with a centromere pattern and negative for antimitochondrial antibody (AMA). The hepatitis panel was negative for viruses A, B, and C. Her serum immunoglobulin G level was 871 mg/dL (normal, <1,600 mg/dL). The rest of the serological tests, including anti-smooth muscle antibodies (ASMA) and anti-liver/kidney microsomal antibodies, were negative. Computed tomography of the abdomen and pelvis without contrast showed normal liver parenchyma and no acute intra-abdominal pathology. Histopathology indicated florid duct lesions. The background parenchyma showed no significant steatosis, and inflammatory changes were limited to the portal areas. Periodic acid-Schiff staining revealed intact hepatic parenchyma and architecture. The patient was diagnosed with AMA-neg PBC and responded well to ursodeoxycholic acid therapy. This case highlights the importance of recognizing AMA-neg PBC as a variant of AMA-pos PBC and differentiating between them. Autoimmune cholangitis is a vague and imprecise condition. All patients with AMA-negative PBC should be tested for other PBC-specific autoantibodies. Although the prognosis and bile duct damage and loss are worse in AMA-neg PBC for unknown reasons, treatment remains the same for both.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"17 1","pages":"14-20"},"PeriodicalIF":0.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b8/68/crg-2022-0017-0001-528437.PMC9895762.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000528437","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
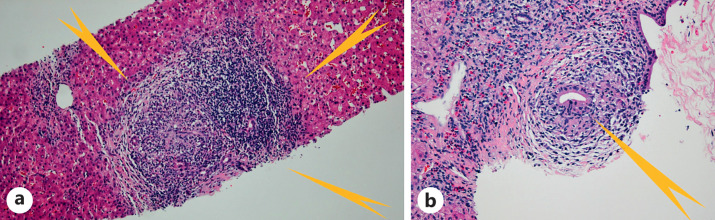
Antimitochondrial antibody-positive primary biliary cholangitis (AMA-pos PBC) is an autoimmune disorder in which monoclonal antibodies are produced against epitopes in the mitochondrial membranes of biliary epithelial cells, resulting in progressive nonsuppurative biliary cholangitis. Up to 5% of patients lack these autoantibodies, termed antimitochondrial antibody-negative (AMA-neg) PBC. Although a somewhat new variant of AMA-pos PBC, it is not an overlapping syndrome. Few studies to date have described this phenomenon. An 87-year-old woman was referred to our clinic with elevated serum alkaline phosphatase (714 U/L). She reported fatigue but no other symptoms. A physical examination revealed a benign lesion and bilateral lower extremity swelling secondary to lymphedema. The serological profile was significant for a high antinuclear antibody titer (>1:2,560) with a centromere pattern and negative for antimitochondrial antibody (AMA). The hepatitis panel was negative for viruses A, B, and C. Her serum immunoglobulin G level was 871 mg/dL (normal, <1,600 mg/dL). The rest of the serological tests, including anti-smooth muscle antibodies (ASMA) and anti-liver/kidney microsomal antibodies, were negative. Computed tomography of the abdomen and pelvis without contrast showed normal liver parenchyma and no acute intra-abdominal pathology. Histopathology indicated florid duct lesions. The background parenchyma showed no significant steatosis, and inflammatory changes were limited to the portal areas. Periodic acid-Schiff staining revealed intact hepatic parenchyma and architecture. The patient was diagnosed with AMA-neg PBC and responded well to ursodeoxycholic acid therapy. This case highlights the importance of recognizing AMA-neg PBC as a variant of AMA-pos PBC and differentiating between them. Autoimmune cholangitis is a vague and imprecise condition. All patients with AMA-negative PBC should be tested for other PBC-specific autoantibodies. Although the prognosis and bile duct damage and loss are worse in AMA-neg PBC for unknown reasons, treatment remains the same for both.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


