{"title":"Conducting Goals of Care Conversations: Lessons From the COVID-19 Pandemic.","authors":"Alison T Lai, Nadine Abdullah","doi":"10.1177/08258597231153386","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective:</b> Internal medicine (IM) residents discuss a patient's goals of care (GOC) as part of their initial consultation. Residents have described inexperience, general discomfort, limited formal teaching, and prognostic uncertainty as barriers to effective GOC conversations. The early COVID-19 pandemic resulted in rapid changes to the healthcare system on the individual, patient, and systemic level that might exacerbate and/or introduce new barriers to IM residents' GOC conversations. This qualitative study examines how the early COVID-19 pandemic challenged IM residents' ability to have effective GOC conversations. <b>Methods:</b> Using a constructivist grounded theory approach, participants (n=11) completed a semi-structured interview. Data collection and analysis occurred simultaneously using an open coding, constant comparison process. Interviews were completed until no new themes were identified. <b>Results:</b> Residents self-described their GOC conversations in 5 steps: normalization of the conversation, introduction of expected clinical course, discussion of possible care plans, exploration of the patient's values, and occasionally providing a recommendation. Residents described limited structured teaching around GOC conversations and instead relied on observed role-modelling and self-practice to hone their skillset. Residents described an increased sense of urgency to have GOC conversations due to the uncertainty of clinical course and potential for rapid deterioration of patients with COVID-19. Residents identified restrictive visitor policies as a significant barrier that contributed to feelings of dehumanization. Residents felt that these limitations affected their GOC conversations and potentially resulted in discordant care plans which contributed to moral distress. <b>Conclusion:</b> The early COVID-19 pandemic resulted in several barriers that challenged residents' ability to conduct effective GOC conversations. This is on the background of previously reported discomfort and limited formal training in conducting GOC conversations. Based on our findings, we present a conceptual model involving teaching validated GOC frameworks, positive role-modelling, and experiential learning to support GOC conversation education in post-graduate medical education.</p>","PeriodicalId":51096,"journal":{"name":"Journal of Palliative Care","volume":" ","pages":"13-20"},"PeriodicalIF":1.7000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/ce/10.1177_08258597231153386.PMC9895296.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Palliative Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/08258597231153386","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/31 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
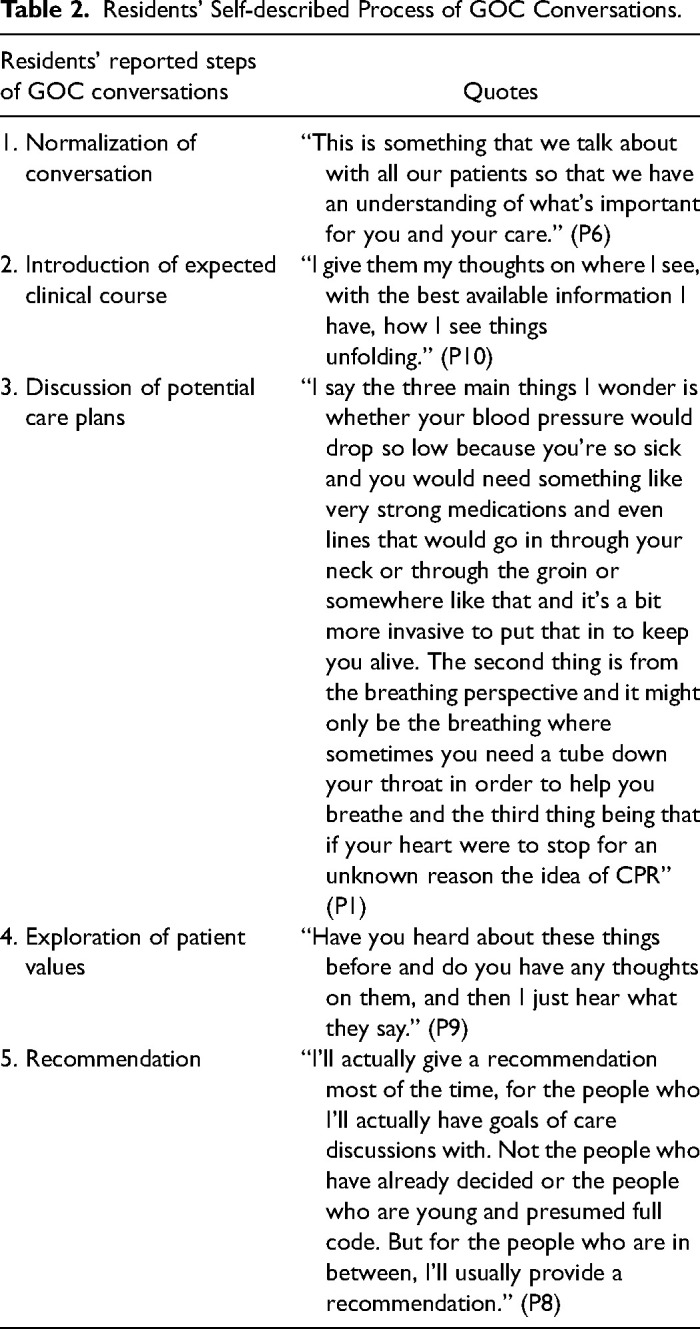
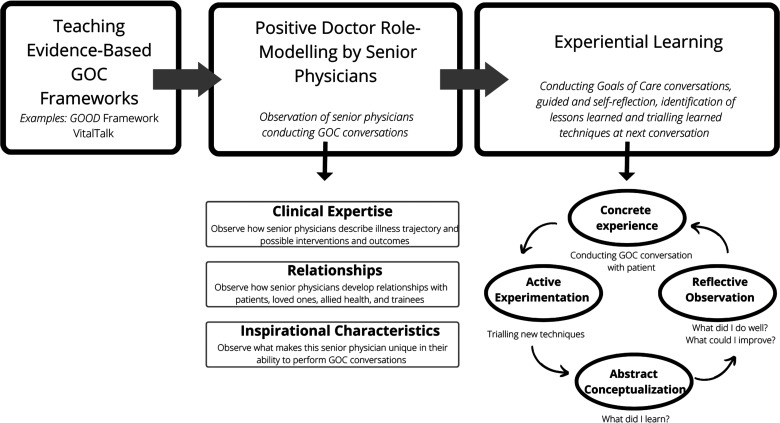
Objective: Internal medicine (IM) residents discuss a patient's goals of care (GOC) as part of their initial consultation. Residents have described inexperience, general discomfort, limited formal teaching, and prognostic uncertainty as barriers to effective GOC conversations. The early COVID-19 pandemic resulted in rapid changes to the healthcare system on the individual, patient, and systemic level that might exacerbate and/or introduce new barriers to IM residents' GOC conversations. This qualitative study examines how the early COVID-19 pandemic challenged IM residents' ability to have effective GOC conversations. Methods: Using a constructivist grounded theory approach, participants (n=11) completed a semi-structured interview. Data collection and analysis occurred simultaneously using an open coding, constant comparison process. Interviews were completed until no new themes were identified. Results: Residents self-described their GOC conversations in 5 steps: normalization of the conversation, introduction of expected clinical course, discussion of possible care plans, exploration of the patient's values, and occasionally providing a recommendation. Residents described limited structured teaching around GOC conversations and instead relied on observed role-modelling and self-practice to hone their skillset. Residents described an increased sense of urgency to have GOC conversations due to the uncertainty of clinical course and potential for rapid deterioration of patients with COVID-19. Residents identified restrictive visitor policies as a significant barrier that contributed to feelings of dehumanization. Residents felt that these limitations affected their GOC conversations and potentially resulted in discordant care plans which contributed to moral distress. Conclusion: The early COVID-19 pandemic resulted in several barriers that challenged residents' ability to conduct effective GOC conversations. This is on the background of previously reported discomfort and limited formal training in conducting GOC conversations. Based on our findings, we present a conceptual model involving teaching validated GOC frameworks, positive role-modelling, and experiential learning to support GOC conversation education in post-graduate medical education.
期刊介绍:
The Journal of Palliative Care is a quarterly, peer-reviewed, international and interdisciplinary forum for practical, critical thought on palliative care and palliative medicine. JPC publishes high-quality original research, opinion papers/commentaries, narrative and humanities works, case reports/case series, and reports on international activities and comparative palliative care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


