Does the clot burden as assessed by the Mean Bilateral Proximal Extension of the Clot score reflect mortality and adverse outcome after pulmonary embolism?
IF 1 Q4 RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
Jostein Gleditsch, Øyvind Jervan, Frederikus Klok, René Holst, Einar Hopp, Mazdak Tavoly, Waleed Ghanima
{"title":"Does the clot burden as assessed by the Mean Bilateral Proximal Extension of the Clot score reflect mortality and adverse outcome after pulmonary embolism?","authors":"Jostein Gleditsch, Øyvind Jervan, Frederikus Klok, René Holst, Einar Hopp, Mazdak Tavoly, Waleed Ghanima","doi":"10.1177/20584601231187094","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rapid diagnosis and risk stratification are important to reduce the risk of adverse clinical events and mortality in acute pulmonary embolism (PE). Although clot burden has not been consistently shown to correlate with disease outcomes, proximally located PE is generally perceived as more severe.</p><p><strong>Purpose: </strong>To explore the ability of the Mean Bilateral Proximal Extension of the Clot (MBPEC) score to predict mortality and adverse outcome.</p><p><strong>Methods: </strong>This was a single center retrospective cohort study. 1743 patients with computed tomography pulmonary arteriography (CTPA) verified PE diagnosed between 2005 and 2020 were included. Patients with active malignancy were excluded. The PE clot burden was assessed with MBPEC score: The most proximal extension of PE was scored in each lung from 1 = sub-segmental to 4 = central. The MBPEC score is the score from each lung divided by two and rounded up to nearest integer.</p><p><strong>Results: </strong>We found inconsistent associations between higher and lower MBPEC scores versus mortality. The all-cause 30-day mortality of 3.9% (95% CI: 3.0-4.9). The PE-related mortality was 2.4% (95% CI: 1.7-3.3). Patients with MBPEC score 1 had higher all-cause mortality compared to patients with MBPEC score 4: Crude Hazard Ratio (cHR) was 2.02 (95% CI: 1.09-3.72). PE-related mortality was lower in patients with MBPEC score 3 compared to score 4: cHR 0.22 (95% CI: 0.05-0.93). Patients with MBPEC score 4 did more often receive systemic thrombolysis compared to patients with MBPEC score 1-3: 3.2% vs. 0.6% (<i>p</i> < .001). Patients with MBPEC score 4 where more often admitted to the intensive care unit: 13% vs. 4.7% (<i>p</i> < .001).</p><p><strong>Conclusion: </strong>We found no consistent association between the MBPEC score and mortality. Our results therefore indicate that peripheral PE does not necessarily entail a lower morality risk than proximal PE.</p>","PeriodicalId":72063,"journal":{"name":"Acta radiologica open","volume":"12 6","pages":"20584601231187094"},"PeriodicalIF":1.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10328056/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta radiologica open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20584601231187094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Rapid diagnosis and risk stratification are important to reduce the risk of adverse clinical events and mortality in acute pulmonary embolism (PE). Although clot burden has not been consistently shown to correlate with disease outcomes, proximally located PE is generally perceived as more severe.
Purpose: To explore the ability of the Mean Bilateral Proximal Extension of the Clot (MBPEC) score to predict mortality and adverse outcome.
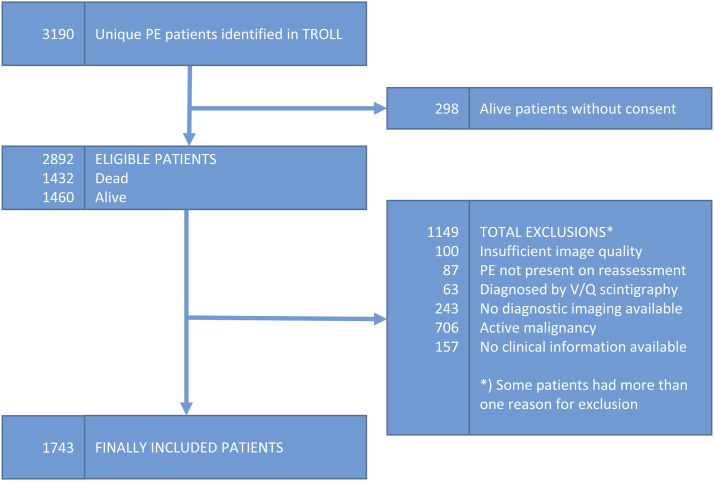
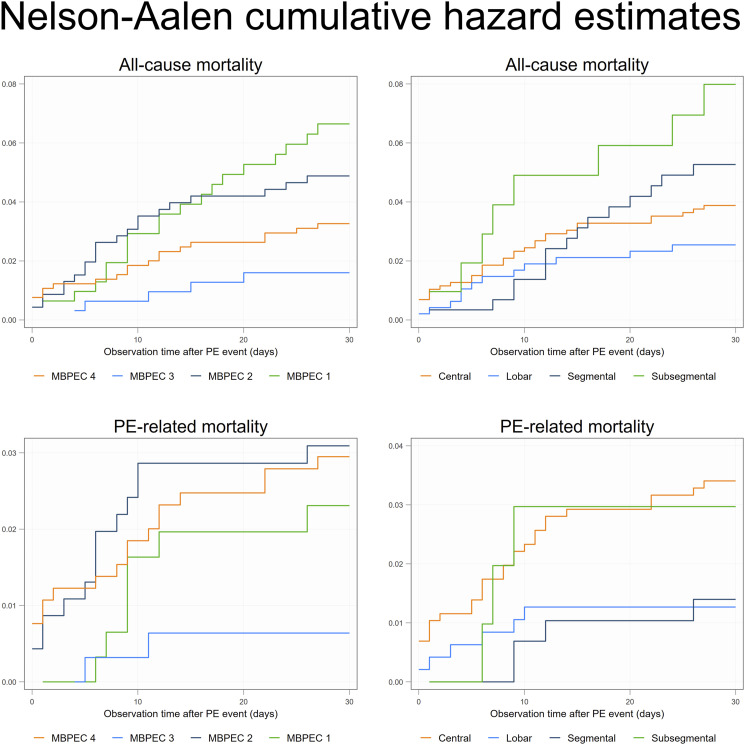
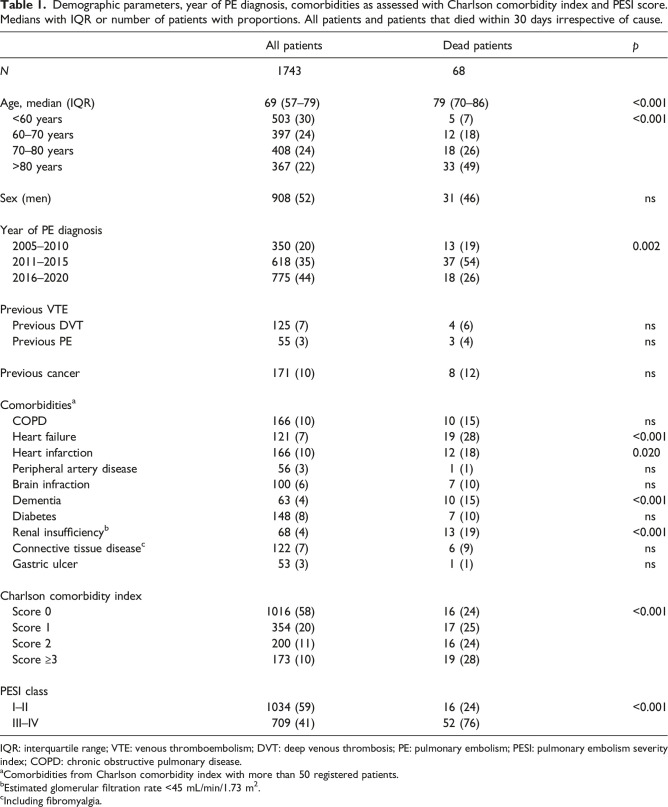
Methods: This was a single center retrospective cohort study. 1743 patients with computed tomography pulmonary arteriography (CTPA) verified PE diagnosed between 2005 and 2020 were included. Patients with active malignancy were excluded. The PE clot burden was assessed with MBPEC score: The most proximal extension of PE was scored in each lung from 1 = sub-segmental to 4 = central. The MBPEC score is the score from each lung divided by two and rounded up to nearest integer.
Results: We found inconsistent associations between higher and lower MBPEC scores versus mortality. The all-cause 30-day mortality of 3.9% (95% CI: 3.0-4.9). The PE-related mortality was 2.4% (95% CI: 1.7-3.3). Patients with MBPEC score 1 had higher all-cause mortality compared to patients with MBPEC score 4: Crude Hazard Ratio (cHR) was 2.02 (95% CI: 1.09-3.72). PE-related mortality was lower in patients with MBPEC score 3 compared to score 4: cHR 0.22 (95% CI: 0.05-0.93). Patients with MBPEC score 4 did more often receive systemic thrombolysis compared to patients with MBPEC score 1-3: 3.2% vs. 0.6% (p < .001). Patients with MBPEC score 4 where more often admitted to the intensive care unit: 13% vs. 4.7% (p < .001).
Conclusion: We found no consistent association between the MBPEC score and mortality. Our results therefore indicate that peripheral PE does not necessarily entail a lower morality risk than proximal PE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


