David Z I Cherney, Alan Bell, Louis Girard, Philip McFarlane, Louise Moist, Sharon J Nessim, Steven Soroka, Sara Stafford, Andrew Steele, Navdeep Tangri, Jordan Weinstein
{"title":"Management of Type 2 Diabetic Kidney Disease in 2022: A Narrative Review for Specialists and Primary Care.","authors":"David Z I Cherney, Alan Bell, Louis Girard, Philip McFarlane, Louise Moist, Sharon J Nessim, Steven Soroka, Sara Stafford, Andrew Steele, Navdeep Tangri, Jordan Weinstein","doi":"10.1177/20543581221150556","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>Kidney disease is present in almost half of Canadian patients with type 2 diabetes (T2D), and it is also the most common first cardiorenal manifestation of T2D. Despite clear guidelines for testing, opportunities are being missed to identify kidney diseases, and many Canadians are therefore not receiving the best available treatments. This has become even more important given recent clinical trials demonstrating improvements in both kidney and cardiovascular (CV) endpoints with sodium-glucose cotransporter 2 (SGLT2) inhibitors and a nonsteroidal mineralocorticoid receptor antagonist, finerenone. The goal of this document is to provide a narrative review of the current evidence for the treatment of diabetic kidney disease (DKD) that supports this new standard of care and to provide practice points.</p><p><strong>Sources of information: </strong>An expert panel of Canadian clinicians was assembled, including 9 nephrologists, an endocrinologist, and a primary care practitioner. The information the authors used for this review consisted of published clinical trials and guidelines, selected by the authors based on their assessment of their relevance to the questions being answered.</p><p><strong>Methods: </strong>Panelists met virtually to discuss potential questions to be answered in the review and agreed on 10 key questions. Two panel members volunteered as co-leads to write the summaries and practice points for each of the identified questions. Summaries and practice points were distributed to the entire author list by email. Through 2 rounds of online voting, a second virtual meeting, and subsequent email correspondence, the authors reached consensus on the contents of the review, including all the practice points.</p><p><strong>Key findings: </strong>It is critical that DKD be identified as early as possible in the course of the disease to optimally prevent disease progression and associated complications. Patients with diabetes should be routinely screened for DKD with assessments of both urinary albumin and kidney function. Treatment decisions should be individualized based on the risks and benefits, patients' needs and preferences, medication access and cost, and the degree of glucose lowering needed. Patients with DKD should be treated to achieve targets for A1C and blood pressure. Renin-angiotensin-aldosterone system blockade and treatment with SGLT2 inhibitors are also key components of the standard of care to reduce the risk of kidney and CV events for these patients. Finerenone should also be considered to further reduce the risk of CV events and chronic kidney disease progression. Education of patients with diabetes prescribed SGLT2 inhibitors and/or finerenone is an important component of treatment.</p><p><strong>Limitations: </strong>No formal guideline process was used. The practice points are not graded and are not intended to be viewed as having the weight of a clinical practice guideline or formal consensus statement. However, most practice points are well aligned with current clinical practice guidelines.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"10 ","pages":"20543581221150556"},"PeriodicalIF":1.6000,"publicationDate":"2023-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9884958/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581221150556","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose of review: Kidney disease is present in almost half of Canadian patients with type 2 diabetes (T2D), and it is also the most common first cardiorenal manifestation of T2D. Despite clear guidelines for testing, opportunities are being missed to identify kidney diseases, and many Canadians are therefore not receiving the best available treatments. This has become even more important given recent clinical trials demonstrating improvements in both kidney and cardiovascular (CV) endpoints with sodium-glucose cotransporter 2 (SGLT2) inhibitors and a nonsteroidal mineralocorticoid receptor antagonist, finerenone. The goal of this document is to provide a narrative review of the current evidence for the treatment of diabetic kidney disease (DKD) that supports this new standard of care and to provide practice points.
Sources of information: An expert panel of Canadian clinicians was assembled, including 9 nephrologists, an endocrinologist, and a primary care practitioner. The information the authors used for this review consisted of published clinical trials and guidelines, selected by the authors based on their assessment of their relevance to the questions being answered.
Methods: Panelists met virtually to discuss potential questions to be answered in the review and agreed on 10 key questions. Two panel members volunteered as co-leads to write the summaries and practice points for each of the identified questions. Summaries and practice points were distributed to the entire author list by email. Through 2 rounds of online voting, a second virtual meeting, and subsequent email correspondence, the authors reached consensus on the contents of the review, including all the practice points.
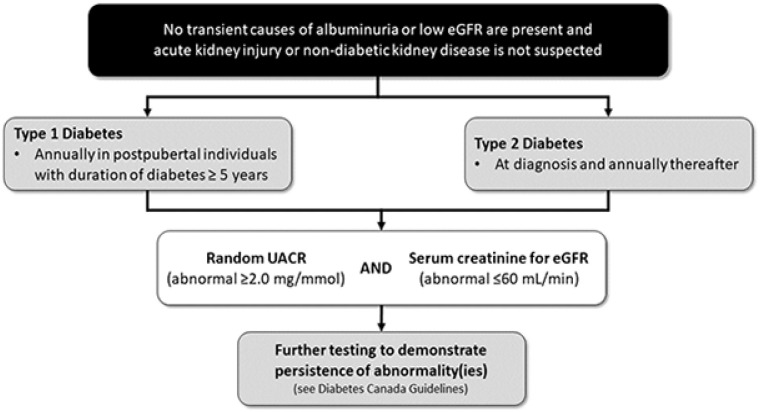
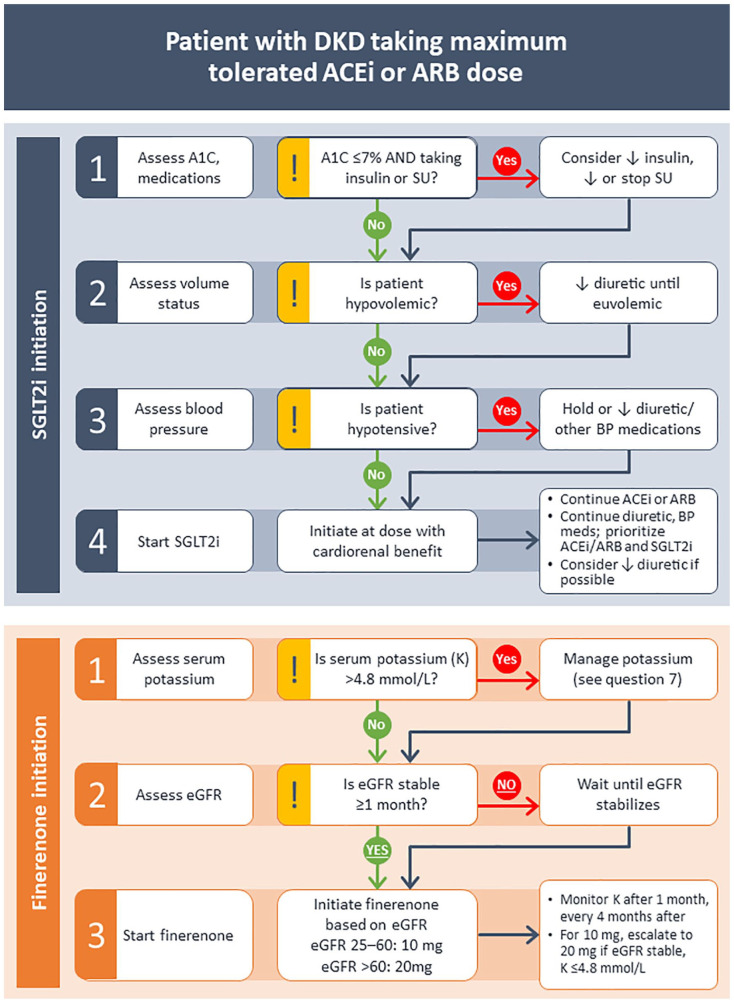
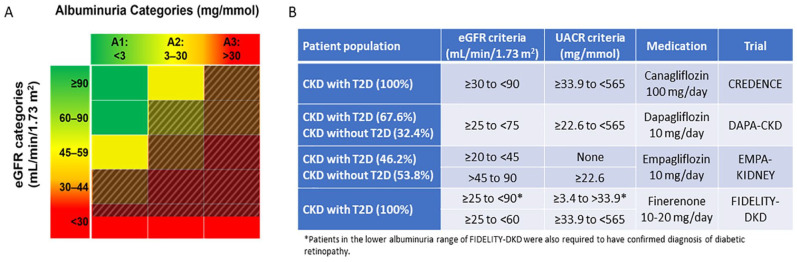
Key findings: It is critical that DKD be identified as early as possible in the course of the disease to optimally prevent disease progression and associated complications. Patients with diabetes should be routinely screened for DKD with assessments of both urinary albumin and kidney function. Treatment decisions should be individualized based on the risks and benefits, patients' needs and preferences, medication access and cost, and the degree of glucose lowering needed. Patients with DKD should be treated to achieve targets for A1C and blood pressure. Renin-angiotensin-aldosterone system blockade and treatment with SGLT2 inhibitors are also key components of the standard of care to reduce the risk of kidney and CV events for these patients. Finerenone should also be considered to further reduce the risk of CV events and chronic kidney disease progression. Education of patients with diabetes prescribed SGLT2 inhibitors and/or finerenone is an important component of treatment.
Limitations: No formal guideline process was used. The practice points are not graded and are not intended to be viewed as having the weight of a clinical practice guideline or formal consensus statement. However, most practice points are well aligned with current clinical practice guidelines.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


